Download
1 / 37
400 likes | 683 Vues
Embolization of Carotid Cavernous Fistulae by transvenous approach through the Facial Vein. Chao-Bao Luo, Michael MH Teng, Feng-Chi Chang, Wan-You Guo Department of Radiology, Taipei Veterans General Hospital and National Yang-Ming University.

E N D
Embolization of Carotid Cavernous Fistulae by transvenous approach through the Facial Vein Chao-Bao Luo, Michael MH Teng, Feng-Chi Chang, Wan-You Guo Department of Radiology, Taipei Veterans General Hospital and National Yang-Ming University
Transvenous embolization of carotid-cavernous fistulae (CCFs) through the inferior petrous sinus (IPS) up to the cavernous sinus (CS) is the common pathway while trans-arterial embolization fail to occlude the fistulae. • Trans-IPS is not always successful because of occlusion/stenosis or difficult anatomy of IPS.
Purpose of the study • To increase the successful occlusion of the CCFs with preservation of the ICA flow (direct type), we present our experiences of trans-facial vein (FV) to embolize CCFs.
Patients and Methods (1) • Over a 5-year period, a total of 76 CCFs were referred to our institute for endovascular embolization. • Among these, 17 patients with CCFs (direct type: 4, indirect: 13) were treated by trans-FV embolization.
Patients and Methods (2) • Trans-FV embolization was selected because of thrombosis/occlusion (n=13), difficult anatomy (n=1) or coil blockage (n=3) of the IPS. • Facial vein drains to external jugular vein in 13, while 4 drains to internal jugular vein. • Trans-femoral vein approach in 16, while direct puncture of jugular vein in 1. • Trans-FV access via superficial facial vein in 16, while one through retromandibular vein. • Detachable coils were selected to embolize in all CCFs.
Results • All CCFs were successfully accessed by trans-FV catheterization; 16 fistulae were totally occluded by detachable coils on immediate angiography. • One residual indirect CCFs spontaneous thrombosis on 6-month follow up. • One direct CCF had a recurrence and was managed by direct puncture of cavernous sinus with coil and NBCA embolization. • There was no significant peri-procedure complication or other recurrent or residual fistula in an average of 9-month follow up.
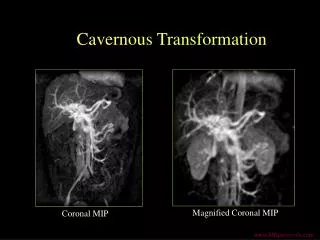
Trans- retromandibular vein, middle temporal vein
F/32y, bruit, chemosis and proptosis of left eye for 5 months
Trans-facial vein embolization of CCFs • A very useful access to CCFs with exclusively anterior drains to SOV and facial vein.
Common venous routes to the CS • Trans-IPS * via ipsilateral IPS * via contralateral IPS >> inter-cavernous sinus • Trans-FV * common FV >> superficial FV>> angular vein >> nasofrontal vein >> SOV * common FV>> retromandibular vein >> middle temporal vein >> nasofrontal vein>> SOV • Trans-SOV: * by surgical exposure or direct puncture
Technique challenge of the trans-FV embolization of the CCFs
1.To found the orifice of the common FV • Choundhry et al (1997) found that 95% FV termination to the internal jugular vein in the level of hyoid bone, only 5% drains to external jugular vein. • In this limited case study, 13 of 17 cases of common FVs drains to external jugular veins. This may lead many error attempts and unnecessary complication.
2.Long courses of facial vein and/or narrow, tortuous courses between angular vein--SOV and SOV--nasofrontal vein around the orbital brim may make catheterization difficult
Trans-facial Vs trans-SOV access to embolize CCFs • Trans-facial approach: * less traumatic route, no require cut-down or puncture of SOV, avoid scars. * may fail due to long and tortuous course. • Trans- SOV approach: * bleeding from SOV, difficult to hemostasis. * injury of supra-orbital nerve, trochlea, levator muscle. * Infection, granuloma.
Conclusions • Knowledge of the varying venous patterns in the neck and facial region is crucial for trans-FV approach of the CCF, in order to avoid any intra-operative error procedure and unnecessary complications. • Trans-FV catheterization is usually successful; it is a safe and effective approach and provides a convenient alternative pathway for transvenous embolization of CCFs when failure to access the fistulae via the IPS.