Download
1 / 47
610 likes | 1.4k Vues
Lateral Elbow Instability. Travis Marion, MD. MSc. BEd . Academic Half Day Apr 2012. Outline. Intro – definitions Anatomy Biomechanics Evaluation Mechanism of injury Acute Terrible Triad Fracture classification Management Reconstruction Priniciples Outcomes

E N D
Lateral Elbow Instability Travis Marion, MD. MSc. BEd. Academic Half Day Apr 2012
Outline • Intro – definitions • Anatomy • Biomechanics • Evaluation • Mechanism of injury • Acute Terrible Triad • Fracture classification • Management • Reconstruction Priniciples • Outcomes • Chronic PRLI • Management • Outcomes
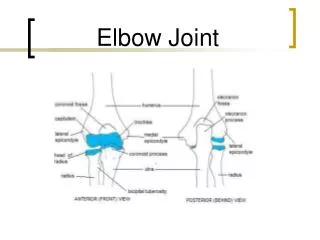
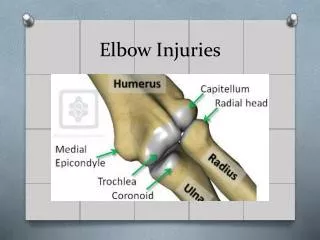
Anatomy Proximal Ulna • Greater sigmoid notch • Lesser sigmoid notch • Sublime tubercle • Coronoid process
Anatomy Coronoid Process • Tip • Body • Anterolateral facet • Anteromedial facet
Anatomy Radial Head • Articulates • Capitellum • Radial notch • Safe Zone2
Anatomy MCL21 • Anterior bundle • Posterior bundle • Transverse
Anatomy LCL19,20 • RCL • LUCL • Accessory lateral collateral • Annular
Biomechanics Primary Stabilizers • Ulnohumeral articulation3 • MCL • LCL complex4 Secondary Stabilizers • Radial capitellar4, 30 • Joint capsule • Common flexor/pronator and extensors • Compressive force • Anconeus, triceps and bracialis • Rotatory stabilizer • ECU, EDM
Evaluation • History • Severity • Mechanism • Precipitants • Chonic • Inciting event • Clicking/snapping/clunking/locking • Apprehensive maneuver • Past medical history • Physical Acute • Inspection • Open vs closed • Alignment • Joint above and below • Detailed neurologic • Physical Chronic • Full pain free ROM • Pain free stressing • Special tests • Closed reduction • Imaging • Radiographs • pre/post reduction • AP/Lat/Oblique • CT
Classification18 • Timing (acute, chronic or recurrent) • Articulations (elbow vs radial head vs both) • Direction of displacement (valgus, varus, anterior, posterolateralrotatory) • Degree of displacement (subluxation or dislocation) – see slide 18 • Simple or complex
Mechanism of Injury • FOOSH, elbow extended • Posteriorly directed force3 • Ulna levers out of trochlea • Valgus stress/posterolateral roll out/supination6 • Capsuloligamentous failure lateral to medial, MCL anterior bundle last to rupture6 • Radial head, coronoidfx
Classification Simple Dislocations • Capsuloligamentous injury • No osseous injury Complex Dislocations • Associated osseous injury
Patterns of Fracture Dislocation • Terrible Triad • Posterior dislocation of radial head • Varusposteromedialrotatory instability • Anterior olecranon fracture dislocations
Fracture Classification Fracture Classification Regan and Morrey7 O`Driscoll8
Traumatic Instability Terrible Triad1 • Elbow dislocation • Coronoid fracture • Radial head fracture
Management Nonsurgical • Concentrically reduced ulnohumeral and radiocapitellar • Stable to allow sufficient ROM (extension to 30°) • Congruency evaluated under fluoroscopically • CT evaluation • Radial head fx minimally reduced with no mechanical block • Type I coronoid fracture • Tx as simple dislocation • Splint at 90° • Isometric biceps/triceps
Management Surgical • Incision • Advantages • Posterior • Access to medial and lateral • Precludes requirement for secondary incision • Reduced injury to cutaneous inervation9 • Improved cosmesis • Disadvanages • Large flaps
Management Kocher • Anconeus (radial) ECU (PIN) EDC split
Management No Replacement • Pros • No healing required • Exposure to coronoid • Faster recovery • Cons • Non anatomic • Overstuffing • Stiffness
Management Yes ORIF • Pros • Anatomic • No overstuffing • Cons • Non union • Malunion • Implant complications • PIN palsy
Management Yes No Medial approach Hotchkiss Can address trochlear fractures Ulnar nerve dissection May address MCL if warranted • One less incision • No ulnar nerve dissection • Amenable to ORIF vs suture technique • Use targeting devices to aid in fixation positioning
Management LCL Repair • Origin at isometric point on lateral epicondyle • Suture anchors vs bone tunnels • Check anatomy • Check stability • If unstable repair the MCL • Persistent instability = external fixator
Reconstruction Principles • < 10% coronoid fractures little effect on stability5 • MCL repair more effective than coronoid repair5 • Most triads involve more than 10% • MCL most important valgus stabilizer • Requires radial head • Radial head acts as buttress • Radial head tensions LCL providing varus stability
Outcomes Pugh and McKee, 2002 • Mean arc 20º and 135º • Mean rotation 135º • Delay in treatment or revision 20% greater loss of motion • 25% revision Pugh et al, JBJS AM, 2004 • 36 patients, multicentred • 112º flexion arc • 136º rotation • 15 excellent, 13 good, 7 fair, 1 poor • 8 revisions (synostosis, instability, contracture release, wound infection) • Prolonged immobilization worse prognosis
Outcomes Frothman et al, J Hand Surgery, 2007 • 30 patients • 117º flexion arc • Rotation 135º • 77% excellent results • Single surgeon, no MCL repairs Similar Findings • Chemama et al, OrthopTraumatolSurg Res, 2010 • Rodriguez-Martin et al, IntOrthop, 2011 • Jeong et al, J OrthopSci, 2010 Lindenhovius et al, J Hand Surgery 2008 • Acute within 2 weeks (ave 6 days) vssubacute repair > 3 weeks (ave 7 weeks) • No difference except 20º more flexion arc
PosterolateralRotatory Instability • Most common type of symptomatic instability • First described 1991 • Recurrent proximal radio-ulnar displacement • Prox radius and ulna rotate externally in relation to the humerus • Radioulnar joint intact and rotates as a single unit as opposed to isolated radial head dislocation
PRLI • Failure of LCL complex • Trauma • iatrogenic • chronic attenuation29 • Physical exam • PRLI - analogous to pivot shift • Table top relocation test
PRLI Radiographs • Avulsion of LCL complex • Degenerative changes • Faber/King lesion (post capitellum lesion analogous to hill sachs) • Drop sign --. Ulnohumeral distance > 4mm on plane lateral
Management Management • Avoid further ligamentous injury • Arthrotomy anterior to LUCL, anterior capsular release • Suture anchor vs lateral ligamentous reconstruction
Outcomes Jones et al, J Shoulder Elbow Surg, 2012 • 8 patients with purely ligamentous PRLI • Surgical graft reconstructionr • Mean f/u 7.1 years • 75% resolution • 25% occasional instability with ADLs Olsen and Sojberg, JBJS Brm2003 • Triceps tendon graft in 18 patients • 4 persistent apprehension • 5 moderate pain Sanchez-Sotelo et al, JBJS Br, 2005 • 12 patients, ligamentous repair, 32 reconstruction • 5 persistent instability (3 from repaired, 2 from recon) • 17 rated excellent • 17 good • 10 fair Similar Findings • Lee and Teo, J Shoulder and Elbow, 2003
References • 1Hotchkiss, Rockwood and Green’s, 1996 • 2Matthew et al, JAAOS, 2009 • 3Mezera and Hotchkiss, Rockwood and Green’s, 2001 • 4Schneeberger et al, JBJS AM, 2004 • 5Beingessner et al, J Shoulder Elbow Surg, 2007 • 6O’Driscoll et al, JBJS, 1991 • 7Regan and Morrey, JBJS AM, 1989 • 8O`Driscoll et al, Instr Course Lect, 2003 • 9Dowdy et al, JBJS BR, 1995 • 10Morrey et al, CORR, 1991 • 11Pugh and McKee, 2002 • 12Pugh et al, JBJS AM, 2004 • 13Frothman et al, J Hand Surgery, 2007 • 14Chemama et al, OrthopTraumatolSurg Res, 2010 • 15Rodriguez-Martin et al, IntOrthop, 2011 • 16Jeong et al, J OrthopSci, 2010 • 17Lindenhovius et al, J Hand Surgery 2008 • 18O’Driscoll, CORR, 2000 • 19Mehta and Bain, JAAOS, 2004 • 20Imatani et al, Jshoulder Elbow Surg, 1999
References • 21Morrey and An, ClinOrthop, 1985 • 22Cohen and Hastings, JBJS Am, 1997 • 23Dunning et al, JBJS AM, 2001 • 24O`Driscoll et al, JBJS, 1991 • 25Jones et al, J Shoulder Elbow Surg, 2012 • 26Sanchez-Sotelo et al, JBJS Br, 2005 • 27Lee and Teo, J Shoulder and Elbow, 2003 • 28Olsen and Sojberg, JBJS Br, 2003 • 29Beuerlein et al, JBJS Am, 2004 • 30Hall and McKee, JBJS, 2005
Nathan L Sacevich circa 1998 • Future ambition: sports medicine doctor • Most memorable experience: losing the soccer championship • Nickname: Nate Dogg • Closet friends: Mack Daddy, Mr Sauce, P Squared (no mention of Travis) • Remembered by: his “stylo” (his style?) • When no one was looking: he liked to get his thug on • People thought: • he looked like a back street boy • “the illest playa”