Download
1 / 132
3.05k likes | 8.27k Vues
Clinical pathology. Dr S Homathy. Pathology The branch of medicine dealing with the essential nature of disease, especially changes in body tissues and organs that cause or are caused by disease. The discipline of Pathology includes both Clinical and Anatomic Pathology. .

E N D
Clinical pathology Dr S Homathy
Pathology • The branch of medicine dealing with the essential nature of disease, especially changes in body tissues and organs that cause or are caused by disease. • The discipline of Pathology includes both Clinical and Anatomic Pathology.
Clinical pathology • pathology applied to the solution of clinical problems, especially the use of laboratory methods in clinical diagnosis.
It is vital for educating physicians to order the correct tests and understand the clinical significance of test results. • The clinician depend upon the laboratory for the diagnosis of diseases • The laboratory plays a crucial role in the diagnosis of disease and therapeutic management of patients.
It is the key subject in the studies of paramedical sciences • It forms bridge between • the preclinical sciences of anatomy, physilogy and biochemistry on one hand and • clinical branches of medical and surgical disciplines on the other
The diagnosis of a disease involves examination of specimens collected from the patients include • urine, • stool, • sputum, • blood, • CSF, • other body fluids and • biopsy material.
The laboratory study of disease by a pathologist using techniques appropriate to the specimen being studied.
Major subspecialty areas in Clinical Pathology are: • Clinical Chemistry/Toxicology • Coagulation • Cytogenetics • Flow Cytometry • Haematology • Haematopathology • Microbiology • Molecular Diagnostics • Transfusion Medicine • Bacteriology, • Chemistry, and • Serology. • Molecular genetics pathology. • In some countries other subspecialties fall under certified Clinical Biologists responsibility • Assisted reproductive technology, Sperm bank and Semen analysis • Immunopathology
Tools of Clinical Pathology • Microscopes, analysers, strips, centrifugal machines... Macroscopic examination • The visual examination of the taken liquid is a first main indication for the pathologist or the physician.
Microscopical examination • Microscopic analysis is an important activity of the pathologist and the laboratory assistant. • They have many different colourings at their disposal (H&E,Gram, Grocott, Ziehl-Neelsen, …). • Immunofluorescence, cytochemistry, the immunocytochemistry and FISH are also used in order make a correct diagnosis. • This stage allows the pathologist to determine the character of the liquid: • “normal”, • tumoral, • Inflammatory • even infectious.
Analyzers • The analysers, by the association of robotics and spectrophotometry, • allowed these last decades a better reproducibility of the results of proportionings, • in particular in medical biochemistry and hematology. • in -vitro diagnosis include chains of automats, • i.e. a system allowing the automatic transfer of the tubes towards the various types of automats of the same mark. • These systems can include the computer-assisted management of a serum library. • These analysers must undergo daily controls to guarantee a result just possible, one speaks about quality control. • These analysers must also undergo daily, weekly and monthly maintenances.
Cultures • A big part of the examinations of clinical pathology, primarily in medical microbiology, use culture media. • Those allow, for example, the description of one or several infectious agents responsible of the clinical signs.
Quality • Laboratories can only produce quality results on quality samples • And on quality requests • Rubbish In - Rubbish Out • Ideal sample mimics the in vivo state
Specimen • Any biological material taken from a patient for diagnostic, prognostic or therapeutic monitoring • Specimens consist • Urine • Stool • Sputum • Wound drainage • Blood • Biopsy material
All samples must be considered to be infectious • Use of “ Universal precautions” handling • Never assume any sample is “ safe”
Phase of analysis • Pre – analytical (from the patient to the lab) • Analytical • Post – analytical (from the lab to the notes)
Pre – analytical (From the patient to the lab) What can and does go wrong • Incorrect identification of patient • Patient preparation • Fasting, diet, supine, time, drugs • Sample poorly/ incorrectly taken • Inaccurate timing • Wrong type of sample
Incorrect containers • Under- filling • Mislabelling/ no labelling • Incorrect storage / transport (ice, warm, delay) • Loss, breakage
The patient • Do patients always disclose history? • Confused • Frightened • In pain • Want to help • Any previous diagnosis available
Patient preparation • Prior to each collection, • review the appropriate test description, • including the specimen type to be collected, • the volume, • the procedure, • the collection materials, and • the storage and handling instructions
Proper sample collection and handling is an integral part of obtaining a valid and timely laboratory test result
Specimens must be obtained using • proper phlebotomy techniques, • collected in the proper container, • correctly labeled (in the presence of the patient) and • promptly transported to the laboratory. • It is the policy of the laboratory to reject samples when there is failure to follow these guidelines. • All specimens should be handled with universal precautions, as if they are hazardous and infectious.
Blood collection • As patients to identify themselves • When blood taken write all relevant details on collection tubes immediately
Other information should include • Ward • Date of collection • Time of collection e.g: cortisol
Patient identification • All patients from whom clinical specimens are obtained must be positively identified prior to specimen collection. • Positive identification is the responsibility of the person collecting the sample.
Identify the patient prior to sample collection, using at least two patient identifiers. • Verify the patient’s name, • unit history number on the identification armband (inpatients), or • drivers’ license or other ID (outpatients) with the information on the requisition.
SPECIMEN COLLECTION TIMING • The basal state (the early morning approximately 12 hours after the last ingestion of food) is recommended for determining the concentration of body constituents such as • glucose, • cholesterol, • triglycerides, • electrolytes, and • proteins.
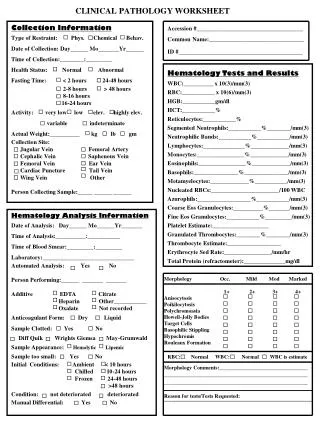
Test request • The test requisition must include: • the patient's name • a unique identification number which assures positive patient identification (e.g., BHT number) • the unit / clinic location • The name(s) and signature of the authorized provider requesting the test(s) • the test(s)/procedure(s) being ordered • the date and time of specimen collection is required on all requisitions • name or initials of person collecting specimen • pager/ phone number of appropriate contact person • office address of requesting physician • diagnosis: ICD9 code or narrative description
Specimen collection • Prioritize collection • "STAT" means special turnaround time and must be collected immediately. • It may involve a patient whose medical condition has suddenly become very critical and must be treated as a medical emergency. • Fasting: Requests for "fasting" specimens are performed before routine requests, so patients can eat meals on schedule.
Order of draw • Blood collection tubes must be drawn in a specific order to avoid cross-contamination of additives between tubes. The recommended order of draw for plastic vacutainer tubes is: • First - • blood culture bottle or tube (yellow or yellow-black top)
Second - • coagulation tube (light blue top). • If just a routine coagulation assay is the only test ordered, then a single light blue top tube may be drawn. • If there is a concern regarding contamination by tissue fluids or thromboplastins, then one may draw a non-additive tube (red top) first, and then the light blue top tube.
Third - • non-additive tube (red top) • Last - additive tubes in this order: • SST (red-gray or gold top): Contains a gel separator and a clot activator. • Sodium heparin (dark green top) • PST (light green top): Contains lithium heparin anticoagulant and a gel separator. • EDTA (lavender top) • ACDA or ACDB (pale yellow top): Contains acid citrate dextrose. • Oxalate/fluoride (light gray top)
Tubes with additives must be filled to their stated volumes and thoroughly mixed. • Erroneous test results may be obtained when the tube is not filled to the stated volume and blood is not thoroughly mixed with the additive. • Mix all tubes with anticoagulant by gentle inversion for 15 seconds.
Types of blood specimens • Venous blood • Capillary blood • Finger prick specimen • Heel prick specimen • Arterial blood
Types of blood samples • Non anticoagulated blood samples • Blood clotting occurs and in 20 min serum can be separated • Anticoagulated blood samples • Na Citrate • Na oxalate • Na/K EDTA • heparin
Red Top/Serum: Chem: all chemistry panels • Thyroid: T3, T4, T-Uptake, TSH • Coronary Risk (CHD): Chol, HDL, LDL • Tumor Markers: PSA, CEA, B-HCG, AFP • Hepatitis:HBsAg, HBsAb, IgM anti-HBc, Hepatitis C, Hepatitis A (HAVAB, HAVAB-M) • Infectious disease molecular tests for RNA or DNA. • AIDS Panel: HIV-1 EIA, Western Blot • Misc: RPR (syphilis), RA screen, nicotine, alcohol, beta-2 microglobulin, CDT
Lavender/Purple Top/EDTA tube: • Anticoaqulant of choice for routine haematologic work • CBC • Molecular test for RNA or DNA • Glycohemoglobin (glycoHB, glycoA1C, Hb A1C) • Sedimentation Rate (ESR) • Reticulocyte Count
An excess of EDTA affects red cells, white cells and platelets causing shrinkage and degenerative changes • Excess of 2mg/ml may result in significant • decrease in packed cell volume and • an increase in mean corpuscular haemoglobin concentration • Mix the anticoagulant and blood by repeated inversion of the container
Blue Top/Sodium Citrate: • PT • APTT • Fibrinogen
Gray Top/Sodium Fluoride: • Glucose, Blood Alcohol Urine: • Urinalysis • Drug Screen
Heparin • Used in the osmotic fragility test and for immunophenotyping • Should not be used to prepare blood films due to faint blue coloration to the background. • Do not use this for WBC as it causes WBC to clump • It does not affect RBC size and less likely to cause haemolysis than EDTA
Tri sodium citrate • It is the choice for coagulation studies • This is the anticoagulant for ESR • 1 volume of sodium citrate is mixed with 4 volumes of blood
Difference between serum and plasma • Serum is obtained from clotted blood that has not been mixed with an anticoagulant • This clotted blood is then centrifuged, yielding serum • Which contain two types of protein:- albumin and globulin • Plasma is obtained from blood that has been mixed with an anticoagulant in the collection tube • Contain:- albumin, globulin and fibrinogen
Sampling problems - blood • Inappropriate site • Drip arm • Mastectomy, burns • Timing • Incorrect use of tourniquet • Wrong container • Incorrect order of draw • Transportation
Urine collection • 24 hour sample must include all urine passed in this period • If less than 24h, inform the lab • Mid stream sample – self explanatory • Early morning sample- often best • Correct container type
Urine samples • Incorrect timing • Inappropriate for test required • Sterility • volume