Download
1 / 31
310 likes | 366 Vues
Aspergillus sinusitis. David W. Denning Wythenshawe Hospital University of Manchester. Patient 1. Presenting features: 3 month history of sneezing and reverse sneezing, left nasal sanguinopurulent discharge, 2 episodes of epistaxis, ulceration of the external left nare,

E N D
Aspergillus sinusitis David W. Denning Wythenshawe Hospital University of Manchester
Patient 1 Presenting features: 3 month history of sneezing and reverse sneezing, left nasal sanguinopurulent discharge, 2 episodes of epistaxis,ulceration of the external left nare, hyperkeratosis of the planum nasale Cécile Clercx in www.aspergillus.man.ac.uk
Nasal endoscopy severe turbinate tissue destruction, presence of multiple fungal plaques in the left nasal cavity and in the left frontal sinus Cécile Clercxin www.aspergillus.man.ac.uk
Treatment of canine nasal aspergillosis 2% imaverol solution infused during one hour through nonsurgically placed catheters Cécile Clercxin www.aspergillus.man.ac.uk
Nasal endoscopy After treatment: absence of fungal plaques, cystic appearance of the left nasal and frontal sinus mucosa severe turbinate tissue destruction, presence of multiple fungal plaques in the left nasal cavity and in the left frontal sinus Cécile Clercxin www.aspergillus.man.ac.uk
Allergic sinusitis Acute invasive sinusitis Interaction of Aspergillus with the hostA unique microbial-host interaction Frequency of aspergillosis Frequency of aspergillosis Chronic invasive sinusitis Fungus ball of the sinus Chronic granulomatous sinusitis Immune dysfunction Immune hyperactivity . www.aspergillus.man.ac.uk
Acute invasive Aspergillus sinusitis Hope et al, Med Mycol 2005:43 (Suppl 1):S207
6 months later after initial caspofungin then voriconazole Myelodysplasia with clinical evidence of sinusitis after chemotherapy – biopsy showed hyphal invasion of bone Pre-treatment www.aspergillus.man.ac.uk
Management of acute invasive Aspergillus sinusitis Requires both biopsy and preferably culture for diagnosis – differential diagnosis = mucormycosis, Scedopsporium/Fusarium infectionRequires systemic antifungal therapy to minimise tissue destruction, including spread to face, eye, mouth and brain and cure
Antifungal treatment of acute invasive Aspergillus sinusitis Herbrecht et al, New Engl J Med 2002; 347:408-15
Antifungal treatment of acute invasive Aspergillus sinusitis First line treatment with voriconazole (n=13) better responses at day 7 of therapy (62% vs 24%), higher CR + PR, better 3-month survival rate (69% versus 38%) fewer severe side effects compared to historical group Rx with amphotericin B or itraconazole (n=21), with or without combined radical surgery. Girmenia and the Girmenia group
Micafungin Favourable response (%) Salvage treatment with caspofungin or micafungin in invasive aspergillosis Caspofungin Maertens et al Clin Infect Dis 2004; 39:1563; Denning et al, J Infect 2006; in press
Management of acute invasive Aspergillus sinusitis Requires both biopsy and preferably culture for diagnosis – differential diagnosis = mucormycosis, Scedopsporium/Fusarium infectionRequires systemic antifungal therapy to minimise tissue destruction, including spread to face, eye, mouth and brain and cure? Requires surgical removal – and if so early or late? Requires granulocytes/other immunotherapy
Chronic invasive Aspergillus sinusitis Hope et al, Med Mycol 2005:43 (Suppl 1):S207
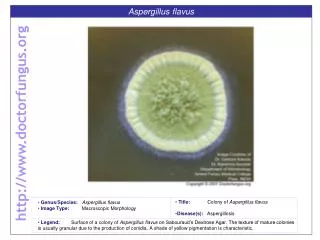
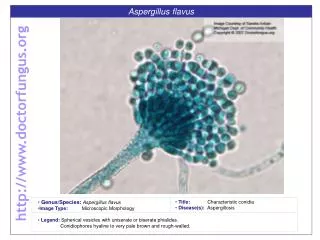
Chronic invasive Aspergillus sinusitis Chronic Aspergillus granulomatous sinusitis = A. flavus Hope et al, Med Mycol 2005:43 (Suppl 1):S207
Diabetic with swelling, nasal obstruction and epistaxis A. terreus cultured ANITHA, NIZAMUDDIN,PUSHPA, REMADEVI. SIHAM 2006
Aspergillus precipitins Probably useful for diagnosis and monitoring response to treatment – but limited data Chakrabarti. Indian J Chest Dis Allied Sci 2000;42:293-304
Allergic Aspergillus sinusitis Clinical features = nasal obstruction, recurrent sinus infections, loss of smell and nasal polyps Aspergillus precipitins +ve in 85% of original series www.aspergillus.man.ac.uk
Surgical handling of specimen very important – mucus versus tissue: allergic or chronic invasive All surgical procedures should be performed without a power microdebrider or the use of suction devices until sample collection is complete. Buzina and the Gras group - www.aspergillus.man.ac.uk /laboratory protocols
Surgical handling of specimen very important – mucus versus tissue: allergic or chronic invasive All surgical procedures should be performed without a power microdebrider or the use of suction devices until sample collection is complete. Mucus should be manually removed, together with inflamed tissue, and placed on a saline-moistened sheet of sterile used x-ray film (approx. 10 x 10 cm) to prevent absorption of the mucus. It should not be placed on a surgical towel or gauze. Buzina and the Gras group - www.aspergillus.man.ac.uk /laboratory protocols
Surgical handling of specimen very important – mucus versus tissue: allergic or chronic invasive All surgical procedures should be performed without a power microdebrider or the use of suction devices until sample collection is complete. Mucus should be manually removed, together with inflamed tissue, and placed on a saline-moistened sheet of sterile used x-ray film (approx. 10 x 10 cm) to prevent absorption of the mucus. It should not be placed on a surgical towel or gauze. Each specimen is then fixed in 10% formalin and embedded in paraffin. Multiple serial sections of different specimens from each patient should be stained with H & E and with GMS. Buzina and the Gras group - www.aspergillus.man.ac.uk /laboratory protocols
Surgical handling of specimen very important – mucus versus tissue: allergic or chronic invasive All surgical procedures should be performed without a power microdebrider or the use of suction devices until sample collection is complete. Mucus should be manually removed, together with inflamed tissue, and placed on a saline-moistened sheet of sterile used x-ray film (approx. 10 x 10 cm) to prevent absorption of the mucus. It should not be placed on a surgical towel or gauze. Each specimen is then fixed in 10% formalin and embedded in paraffin. Multiple serial sections of different specimens from each patient should be stained with H & E and with GMS. The pathologists should pay special attention to the mucin, focusing on fungal elements and eosinophils. Buzina and the Gras group - www.aspergillus.man.ac.uk /laboratory protocols
Chronic invasive Aspergillus sinusitis Complications: - orbital apex syndrome - generalised proptosis and blindness - cavernous sinus thrombosis - osteomyelitis of the base of the skull - cerebral aspergillosis
Orbital apex syndrome Clinical features = sudden or subacute loss of vision, with ophthalmoplegia on one eye, typically associated with sphenoid sinusitis www.aspergillus.man.ac.uk
Base of skull osteomyelitis Clinical features = headache, general ill-health, raised inflammatory markers, sometimes associated sinus features Swift & Denning. J Otol Laryngol 1998;112:92-97.
Sphenoid sinusitis leading to local spread to the brain and cerebral aspergillosis Sphenoid sinusitis causes a band-like headache over the vertex of the skull, and major deterioration in headache. Nasal symptoms often absent, but loss of smell common. www.aspergillus.man.ac.uk
Non-allergic Aspergillus sinusitis Hope et al, Med Mycol 2005:43 (Suppl 1):S207
Saprophytic Aspergillus sinusitis www.aspergillus.man.ac.uk
Saprophytic maxillary Aspergillus sinusitis Often follows upper jaw root canal work, with the use of zinc materials, and penetration of the sinusPresents with ‘chronic’ or ‘recurrent’ sinusitisRequires removal of fungal ball, and creation of an antrostomy. Surgical biopsy of the mucosa required to distinguish chronic invasive disease from saprophytic. Antifungal therapy not required
Conclusions The same spectrum of Aspergillus disease in the lung is found in the sinusesBony erosion is consistent with all formsThe pace/rapidity of the disease is a good guide to the severityHistology of mucosa and mucous key to determining disease classification and managementPrecipitating antibodies useful in diagnosisTreatment depends on the type of disease