Download
1 / 20
210 likes | 373 Vues
My Chest Hurts. Shalini Chandra MD January 26, 2005. Case History.

E N D
My Chest Hurts Shalini Chandra MD January 26, 2005
Case History • 12 year-old boy hero was fighting in his first of three matches at the state wrestling finals when he was ruthlessly thrown to the mat, landing onto his chest. Fortunately, he did not lose consciousness, did not have any head injury, did not have difficulty breathing or swallowing, but had severe chest pain…nonetheless….
…our young hero had his pride at stake, so he decided to be tough and fought not one…but two more matches…and despite his injury he won a fourth place medal! When asked about pain, he said it hurt at first but then he didn’t think about it. When asked about sensory loss, he said after the tournament, he noticed a little tingling in his fingers, but as long as he keeps his elbow bent it is okay. He had also noted it to be slightly blue, but this too has since resolved.
Hospital Course Our patient was taken to an outside hospital first, where an x-ray and a ct scan were done. The films were read as a posterior sternoclavicular joint dislocation. The physicians, promptly put the hero’s right arm in a figure 8 sling and sent him to the one…the only…Penguin Pod at CHM!
Hospital Course Here, at CHM, we promptly collected the films brought to us by our hero himself. The SC joint did not look quite right. We examined our patient. We did not remove the sling, however his arm was pink, and his sensation perfect…even at the tips of his little fingers. We were able to illicit pain on palpation of the upper right sternal border, and mild neck tenderness upon turning neck to the left.
Hospital Course We promptly notified the orthopedic surgeon on call of the situation who requested us to have the films read by our radiologist, and if indeed the dislocation was greater than one centimeter, he would reduce it. Although he initially denied pain, since he had received motrin at the outside hospital, he did eventually ask for some more motrin. We granted his wish. Then we waited for the surgeon and the radiologist to give their verdict…
The Story so far… The SC joint was indeed separated and moderately sprained but not dislocated completely…ie it was less than 1cm displaced, thus no further intervention was needed and our superhero went home with the sling and was to follow-up with orthopedic surgery in 7-10 days to reassess and begin increasing range of motion. He will likely return to sports upon regaining full and pain-free range of motion.
Sternoclavicular Joint Dislocation
What is it? An unusual dislocation at the sternoclavicular joint that is usually the result of compressive forces on the shoulder girdle. The forces of posterior compression transmit through the fulcrum of the costoclavicular ligament and result in posterior dislocation. Alternatively, a direct blow to the anteromedial clavicle can result in posterior dislocation.
Who Gets it? • Ice Hockey Players • Lacrosse Players • Wrestlers • Male Gymnasts • Football Players • Soccer Players
Know thy enemy… • Direct trauma to the great vessel origins, or brachiocephalic vein. Mediastinal hematoma is usually present • Respiratory distress from compression on the trachea • Voice change from compression of the recurrent laryngeal nerve • Pneumothorax
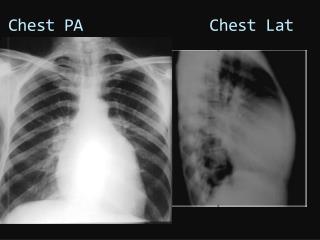
How do we see it? • Special plane film views are an option, but few people know the technical aspects of shooting these films, and even fewer can read them, so… • CT is the modality of choice because it delineates the anatomy of the joint so well, shows the degree of separation, and can also show vascular or other organ injuries • If clinical suspicion is high... go directly to CT
How do we treat it? • Mild and moderate sprain, • treatment is symptomatic and conservative. A sling or figure-of-eight harness can reduce stresses on the SC joint and prevent subluxation. • After 7 to 10 days, range-of-motion exercise is initiated. Return to sports is allowed when the athlete has no pain and full range of motion and can perform sport-specific movements without limitation.
How do we treat it? • Anterior dislocations can be easily reduced with the patient supine and a rolled towel placed between the scapulae. Traction and abduction on the arm with direct pressure on the clavicle will generally reduce the dislocation. The reduction is often unstable, but an anterior dislocation can be left unreduced after an initial attempt with little functional deficit.
How do we treat it? • Posterior dislocations require reduction due to high risk of complications. • If the patient is skeletally mature, closed reduction should be attempted in the OR under anesthesia. • Occasionally, conversion to an anterior dislocation is the treatment of choice. If that fails, open reduction may be indicated. • Younger patients (<22yo) with an open proximal physis may not need open reduction because of bony remodeling potential • Following reduction, follow anterior dislocation instructions.