Download
1 / 110
1.12k likes | 1.32k Vues
Introduction to the Topics: Setting the Stage. Advisory Committee for Pharmaceutical Science and Clinical Pharmacology March 18-19, 2008 Rockville, Maryland. Lawrence J. Lesko, Ph.D., FCP Director, Office of Clinical Pharmacology Center for Drug Evaluation and Research

E N D
Introduction to the Topics: Setting the Stage Advisory Committee for Pharmaceutical Science and Clinical PharmacologyMarch 18-19, 2008Rockville, Maryland Lawrence J. Lesko, Ph.D., FCP Director, Office of Clinical Pharmacology Center for Drug Evaluation and Research Food and Drug Administration Silver Spring, Maryland, USA
Topic 1. Clinical PGx – Rationale for Exploratory Analysis in Early Drug Development • Differences in in pharmacokinetics (PK) and systemic exposure of a drug, or its active metabolite, are related to genetic variation in one or more CYP450 enzymes or transporters • Differences in systemic exposure can potentially lead to significant changes in relevant biomarkers and/or clinical endpoints • Genetic polymorphisms in drug targets may potentially cause important differences in pharmacodynamics (PD) • There are various options available to evaluate differences in PK and/or PD due to gene variants • Genotyping may potentially be needed to stratify dosing in subsequent clinical trials
Proposed Draft Clinical PGx Guidance • Objective To assist the pharmaceutical industry, who are conducting new drug development – or who are involved with relabeling of previously approved drugs – in how to assess the interindividual variability in PK and/or PD that may be caused by known polymorphisms in genes related to ADME and drug targets. Clinical PGx studies have implications for preparing informative drug labels.
Why Now? • Numerous genomic biomarkers affecting PK and/or PD have now been well characterized • Cost-effective technology exists to explore lesser known gene variants affecting ADME and PD • Other FDA Clinical Pharmacology guidances refer to PK/PD related to PGx without being specific • European and Japanese regulatory authorities have published preliminary guidance on clinical PGx • ICH PGx WG at Step 5 on E15 and will continue to focus on harmonization topics
Collection of DNA for Exploratory Analysis in Early Drug Development • Rationale • It is not always known why similar healthy volunteers or patients experience unusual exposures, serious adverse events or no clinical response following drug administration • Current thinking is that there may be a genetic basis for such differences • Clinical studies provide a major opportunity to collect and store biological samples for DNA analysis to investigate these differences
Topic 2. Quantitative Clinical Pharmacology: Drug-Disease Models As a Critical Path Research Opportunity • FDA is working with public-private partnerships, industry and academia to evaluate the feasibility of developing drug-disease models • The long-term goal is to develop models that can potentially be used to design better clinical trials, predict adverse events and optimize dosing • Drug-disease models have the potential to identify which subset of patients are most likely to receive benefit or be harmed • Drug-disease models may potentially improve productivity in therapeutic areas with high clinical trial failure rate • NSCLC represents one such model
Pediatrics: A Pilot Project for Leveraging Prior Knowledge and Quantitative Clinical Pharmacology • ObjectiveTo find better ways to use existing knowledge about age-related PK and/or PD differences and quantitative methods to improve:1. dose selection for pivotal pediatric clinical studies2. other design features for pediatric clinical studies3. quality of pediatric written requests4. information about pediatrics in drug product labels
Topic 3. Renal Impairment Concept Paper – Rationale for Updating the 1998 Guidance • Premarketing observations – renal impairment causes significant changes in systemic exposure beyond those drugs cleared only by renal pathways • Quantitative assessment of drug metabolism and/or transport in renal impairment may avoid potential advese events related to changes in drug PK and/or PD profiles • The 1998 guidance was silent on premarketing studies to assess how hemodialysis would influence drug exposure leading to uncertainty in dosing • An update of the guidance will assist the pharmaceutical industry, based on contemporary evidence and expert input, in conducting informative premarketing renal impairment studies
New Concept Paper/ Guidance on Clinical Pharmacogenetics Clinical Pharmacology Advisory Committee Rockville, MD March 18, 2008 Felix W. Frueh, PhD Associate Director for Genomics Office of Clinical Pharmacology CDER/FDA
Background • Rapid increase in our understanding about the role of genetic variations in human germline DNA in inter-individual differences in exposure-response relationships: • while studying well characterized allelic variations in e.g. drug metabolizing enzymes, transporters, and certain drug targets allow us already today to address a sizeable amount of this variation, • new molecular technologies enable us to learn more about the pharmacokinetics (PK) and pharmacodynamics (PD) about therapeutics.
Background, cont’d • FDA issued a “Guidance for Industry: Pharmacogenomic Data Submissions” in 2005. This guidance: • Creates a broadly applicable, general framework of regulatory aspects concerning the use of genomic and genetic biomarkers in drug development • Clarifies what type of genetic or genomic data needs to be submitted and when • Introduces a novel pathway (VGDS) for submitting early stage, exploratory data which is not ready for use in regulatory decision making • Encourages the conduct and submission of such data under the VGDS program
Background, cont’d • “Guidance for Industry: Pharmacogenomic Data Submissions” does not discuss in detail • The decision making process itself • The design of studies using pharmacogenetic information • The implications of the use of pharmacogenetic information on the drug label
Scope • This new concept paper/ draft guidance on clinical pharmacogenetics will discuss • Our current view on whether or not clinical pharmacogenetic studies should be performed or not based on the amount of information at hand • General strategies to use pharmacogenetic information in drug development • The design of clinical pharmacogenetic studies • The implications of the results of these studies on the drug label
Outline/ Content • Introduction • General Strategies • Decision Tree for Integrating Pharmacogenetic Studies into the Drug Development Process • In Vitro Studies Evaluating Drug as Substrate for Polymorphic Genes to Guide Clinical Studies • Design of Clinical Pharmacogenetic Studies • Labeling Implications • References
Outline/ Content • Introduction • General Strategies • Decision Tree for Integrating Pharmacogenetic Studies into the Drug Development Process • In Vitro Studies Evaluating Drug as Substrate for Polymorphic Genes to Guide Clinical Studies • Design of Clinical Pharmacogenetic Studies • Labeling Implications • References
General Strategies • Exploring the feasibility of using pharmacogenetic information for adjusting the dose, or to identify responders/ non-responders requires the (prospective) collection of DNA samples • We recommend to collect and bank DNA samplesfrom all participants in clinical trials • This information should be used as early as possible and carried forward into the later stages of drug development as appropriate • We recommend to conduct pharmacogenetic studies in early drug development
Considerations for Conduct of PGt Studies in Early Drug Development • Entry criteria based on genetics can be established as early as Phase 1 (e.g. when pre-clinical studies suggest that a molecule is metabolized by a polymorphic pathway, clinical pharmacokinetic studies should be performed in healthy volunteers to determine the differences in exposure related to genotype) • Phase 1 and 2A studies are often exploratory because of small sample sizes and lack of statistical significance • However, these can be important studies for hypothesis generation to define subsets for dosing or identify responders/ non-responders • Associations between a marker of interest and an outcome found in such studies generally require confirmation through study replication • Banked samples (from all stages of development) can also be important for exploring unexpected safety signals
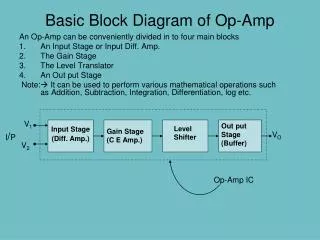
Decision Tree • Goal: To assist in the integration of pharmacogenetic studies early into the drug development process
Molecule (NME) Pre-clinical: in vitro metabolism and/or transporter studies on well characterizedcandidate genes (e.g. CYP2C9, CYP2C19, CYP2D6, UGT1A1, etc.) NME is a known substrateof a polymorphic enzyme: <25%of total metabolism or clearanceaffected NME is a known substrateof a polymorphic enzyme: >25% of total metabolism or clearance affected NME is not a substrate, or unknownto be a substrate of a well characterized polymorphic enzyme Collect DNA in Phase 1 – 2 studies STOP: Label appropriately Collect DNA in Phase 1 – 2 studies Screen of DNA for panel of gene variants of metabolism and transport and sources of PK or PD variability allows to generate hypothesis Is difference between genotypes (PM vs. EM,or from an inhibitiondrug-interaction study) in PK important and based on dose-response or PK/PD data? Select genotype-driven doses for Phase 2B – 3 or dose adjustment in label based on genotype Yes Yes No Consider VGDS Label appropriately Collect DNA in future clinical trialsto evaluate outliers, study adverseevents or efficacy failures No Collect/ bank DNA for future exploratory or hypothesis generating studies STOP STOP: Label appropriately
Design of Clinical Pharmacogenetic Studies – Purpose of Studies • The objective of clinical pharmacogenetics studies is to understand the importance of genetic factors in explaining and predicting inter-individual differences in drug exposure and response • Usually, this requires well-designed prospective studies to assess the pharmacokinetic and pharmacodynamic properties associated with genetic variations
Design of Clinical Pharmacogenetic Studies – General Considerations • A clinical pharmacogenetics study can be performed as an independent study or as an add-on to a larger clinical trial • The sample size of the study will depend on the purpose of the study, and the acceptable error rates (type 1 and type 2 errors) to define the variability • A specific clinical pharmacogenetic study may be warranted based on pre-clinical data • Studies can be conducted sequentially during drug development to refine the question and maximize the understanding of the biomarker • To be meaningful, clinical pharmacogenetic studies should be performed using analytically validated methods and include appropriate controls
Design of Clinical Pharmacogenetic Studies – Study Populations • Phase 1 studies are usually conducted in healthy volunteers • However, under certain circumstances safety considerations may preclude the use of healthy volunteers (e.g. anticancer drugs) • Exclusion of subjects from clinical trials may be appropriate when it is known that subjects with certain genotypes would not respond favorably, or if there is a specific safety concern (e.g. due to high exposure) • Ethnicity may be an important co-variate for consideration in cases where allele frequencies vary between ethnicities and the effect of these variations may influence biological processes related to the therapy
Design of Clinical Pharmacogenetic Studies – Study Types, cont’d
Design of Clinical Pharmacogenetic Studies – Study Types, cont’d
Design of Clinical Pharmacogenetic Studies – Study Types, cont’d
Design of Clinical Pharmacogenetic Studies – Study Types, cont’d
Question to the Committee • It is proposed to collect DNA samples from all participants in clinical trials. • What issues or barriers should be addressed to facilitate routing collection of DNA samples? • When (under what circumstances, to what degree) should DNA be collected during drug development for use in exploratory analysis? • A decision tree depicting the integration of pharmacogenetic studies into the drug development process is proposed. • What comments and/or recommendations does the committee have on the scientific rationale and thought process embodied in the proposed decision tree? • Different study types for clinical pharmacogenetic studies are proposed. • What comments and/or recommendations does the committee have on the design of clinical pharmacogenetic studies and their proposed impact on subsequent clinical trials?
Leveraging Prior Quantitative Knowledge to Guide Drug Development Decisions Joga Gobburu Director, Pharmacometrics Office of Clinical Pharmacology OTS/CDER/FDA jogarao.gobburu@fda.hhs.gov Gobburu, Pharmacometrics
Quantitative Clinical Pharmacology: Critical Path Opportunity Gobburu, Pharmacometrics
Pharmacometrics (or Quantitative Experimental Medicine) • Science that deals with quantifying disease and pharmacology to influence drug development and regulatory decisions • Focus is on ‘learning’ rather than ‘confirmation’ • Diverse Expertise Needed • Quantitative (Clinical) Pharmacologists, Clinicians, Statisticians, Bioengineers Gobburu, Pharmacometrics
Diverse Expertise FDA Data • Biology • Natural Progression • Placebo • Biomarker-Outcome • Pharmacology • Effectiveness • Safety • Early-Late • Preclinical-Healthy-Patient • Patient Population • Drop-out • Compliance Physiology Prior Quantitative Knowledge Disease Model Drug Model Trial Model Disease-Drug-Trial models are collectively called as Disease Models Gobburu, Pharmacometrics
Diverse Expertise FDA Data Dose Selection Patient Selection Physiology Prior Quantitative Knowledge Disease Model Drug Model Trial Model Molecule Screening Trial Design Gobburu, Pharmacometrics
FDA Disease Models: Highlights Gobburu, Pharmacometrics
FDA Disease Models: Highlights Gobburu, Pharmacometrics
Disease Models: Questions • 1. What comments or suggestions does the committee have for improving the mathematical, statistical or clinical concepts in the model? • 2. How does the committee envision such a model can be best utilized to improve drug development? • 3. Does the committee have any general recommendations for further exploratory research into drug disease models? Gobburu, Pharmacometrics
Pediatric Initiative: More Efficient Trials • Experience dictates that pediatric trials could be designed to render more useful information • Goal is to employ prior knowledge from adults/pediatrics (using disease models) to design future pediatrics written request studies Gobburu, Pharmacometrics
Disease Model Drug Model Trial Model Inter-disciplinary Team Governance Committee WR Data (adult/ped) Industry E-Library Communication Pediatric Initiative: Conceptual Framework Gobburu, Pharmacometrics
Designing Pediatric Trials: Questions • 1. Do you think that such an approach will render pediatric trials more informative with respect to better dosing and study designs given the difficulties in conducting pediatric clinical trials? • 2. Given limited resources, please advice us on how to prioritize pediatrics programs for applying model-based trial design? • 3. Do you have any suggestions on how to improve the approach with respect to closing our knowledge gaps in pediatric pharmacotherapy? Gobburu, Pharmacometrics
An Example of Disease Model (NSCLC) Clinical Pharmacology Advisory Committee (CPAC) March 18-19, 2008 Yaning Wang, Cynthia Sung, Celine Dartois, Roshni Ramchandani, Brian Booth, Ed Rock and Joga Gobburu Office of Clinical Pharmacology Office of Translational Sciences Center for Drug Evaluation and Research Food and Drug Administration
Basic Facts Cancer Death Rates in US Female Male Cancer Facts & Figures 2006, American Cancer Society
Low Success Rate in Oncology Kola I, Landis J.Can the pharmaceutical industry reduce attrition rates? Nat.Rev.Drug.Disc. Aug 2004.
High Failure Rate Even Phase III Kola I, Landis J.Can the pharmaceutical industry reduce attrition rates? Nat.Rev.Drug.Disc. Aug 2004.
Objective • Generate quantitative information that can be shared to improve oncology drug development • Risk factors for survival • Disease model for tumor size change over time • Quantitative relationship between tumor size related metrics (early biomarker) and overall survival Note: Exploratory tool, not intended for surrogate endpoint
Perceived Utility of Models • Decrease attrition rate • by allowing better screening of compounds early in development • Optimize dose selection • by targeting meaningful changes in tumor size & balancing toxicity • Increase trial success rate • by aiding in designing better survival trials
Database • Four registration trials (A, B, C, D) for non-small cell lung cancer (NSCLC) • Eight active treatments and one best supportive care (placebo) • First-line or second line treatment for locally advanced or metastatic NSCLC (stage IIIA/B, IV) • N=243-488/arm
Risk Factors Evaluation • Risk factors tested • Degree of weight loss over the previous 6 months (< 5% vs. ≥ 5%) • ECOG performance status (0 + 1 vs 2 + 3 or 0 vs 1) • Prior surgery (Yes or No) • Prior radiation (Yes or No) • Prior chemotherapy (Yes or No) • Best response to prior therapy (complete response [CR] or partial response [PR] vs stable disease [SD] vs PD) • Sex • Age • Baseline tumor size (sum of longest dimensions) • Number of prior chemotherapy • Lactate dehydrogenase (LDH>ULN) • Method • Cox regression (stepwise, inclusion 0.1, exclusion 0.05)
Disease Model for Tumor Size A mixed exponential and linear model f(t): sum of longest dimensions (SLD) at time t A: SLD at time 0, cm k: SLD decay rate (treatment dependent), 1/week B: SLD growth rate (treatment dependent), cm/week Between subject variability for A, k and B (random effect): Note: dose/exposure effect can be added to k and B if data are available
Database for Tumor Model • 20-30% patients without post-baseline tumor measurements • Distribution of time for tumor measurements