Download
1 / 22
320 likes | 683 Vues
RTOG1106: Randomized Phase IIR Trial of Personalized Adaptive Radiotherapy Based on Mid-treatment FDG-PET in Locally Advanced NSCLC. P.I.: Feng-Ming (Spring) Kong, M.D., Ph.D. Study Team Mitchell Machtay, M.D. Jeffrey D. Bradley, M.D. Jean Moran, Ph.D. Vera Hirsh, M.D. Barry Siegel, M.D.

E N D
RTOG1106: Randomized Phase IIR Trial of Personalized Adaptive Radiotherapy Based on Mid-treatment FDG-PET in Locally Advanced NSCLC P.I.: Feng-Ming (Spring) Kong, M.D., Ph.D. Study Team Mitchell Machtay, M.D. Jeffrey D. Bradley, M.D. Jean Moran, Ph.D. Vera Hirsh, M.D. Barry Siegel, M.D.
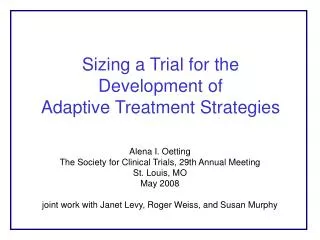
RTOG 1106/ACRINxxxx RTOG 0617 arm: Standard dose script Study arm: Individualadaptive RT Estimated Sample size: ~120 patients (85% power to detect 20% difference in 2-yr. local PFS)
Background - 1 The Traditional Approach CT 1-3 months PET Treatment including Radiation Therapy post-treatment outcome Weeks to months Months to years
ACRIN 6668/RTOG 0235: FDG-PET 2-3 months after XRT REGISTER Eligibility Stage III NSCLC plan for conc. chemo-RT PS 0-1 Chemo-RT +/- ‘adjuvant’ chemo FDG-PET with SUV FDG-PET with SUV Primary Endpoint: Survival as a function of post-RT SUV Sample Size: 250
ACRIN 6668/RTOG 0235 Update • Activation Date: 3/1/2005. • Closed to Accrual: 5/15/2009. • Total Accrual: 251 pts. • 236 verified eligible (94%). • Total # Participating Sites: 37. • Central Review in Process. • Qualitative, SUVpeak, MTV • Primary Outcome Analysis in Early/mid 2011.
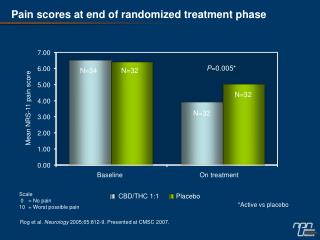
RTOG 0515 Results Exploratory trial of pre-Tx FDG-PET for XRT planning N=47 Bradley et al. ASTRO 2009
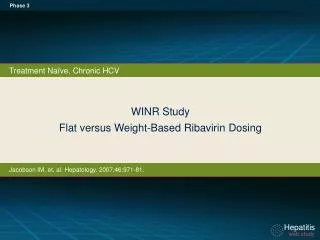
Hypotheses • Use of mid-treatment FDG-PET is as useful or more useful than pre-RT FDG-PET and/or 3-month post-RT PET. • Mid treatment PET can be used to individualize (and escalate) XRT dose will result in improved outcomes (2-yr. LPFS) compared with standard XRT.
When should PET be done? The Traditional Approach CT 1-3 months PET • Post-RT PET response is highly correlated with pathologic response. • Post-RT PET is predictive of long term survival and pattern of failure • (Mac Manus et al, 2003) • RTOG235/Acrin688 results awaited. Treatment including Radiation Therapy post-treatment outcome However, post-RT PET tumor response does not provide an opportunity to change the treatment plan. Weeks to months Months to years
PET during RT? • PET scan can be performed during-RT • University of Michigan study, ASTRO 2005 • MAASTRO study, ASTRO 2005 • Stanford study, ASTRO 2007 • Princess Margaret Hospital, ASTRO 2008 • UM has demonstrated that PET response at 45 Gy during-RT was highly correlated with post-RT response in a small pilot study. • The above finding has been recently validated in another 50+ patients from Michigan. Kong et al, JCO, 2007
Individualized RT Escalation Is Feasible Michigan trial usees PET-MTV guided isotoxicity adaptive plan to escalate tumor dose: 30 daily treatments, 2.2-3.8 Gy per fraction, 66 Gy~85.5 Gy To NTCP of 17% (mean lung dose 20 Gy), with concurrent and adjuvant carbo and taxol, maximum at102 Gy in 2 Gy equivalent dose for lung (=ED2) (92 Gy ED2 for tumor). 14 patients completed treatments per study, all patients treated >74 Gy ED2 (median=92 Gy for tumor), majority of them received the maximum dose. 6 patients followed up for 1.5 years, no local failure thus far, 2 brain mets, only 1 death thus far from GI bleeding (gastric and esophageal ulcers).
Tumor Response During-RT Tumor Pre- RT Tumor Heart During-RT at 45 Gy Tumor Tumor Heart Example-1
CT-lunGwindow CT-mediastinum window UM002 FDGPET Pre-RT GTV: 468 cm3 MTV: 353 cm3 During-RT GTV: 402 cm3 MTV: 268 cm3 3 mo post GTV: 174 cm3 MTV: 12 cm3 This 48 YO male received 85.5 Gy (120 Gy BED) had grade 0 clinical toxicity thus far. He works full time now with heavy duty. 9 mo post 16 mo post Patient-2
FDG Activity & PET-MTV Reduction PET results during RT correlates well with post-RT results
PET-MTV Decreased More than CT-GTV 50 pts 88 tumors CT PET During-RT Pre-RT During-RT
Mid-course FDG-PET and PFS 1 Year Progression-Free Survival (Kong et al, ASTRO 2009)
Mid-course FDG-PET and Survival Local Progression Free Survival Overall Survival NSUV During-RT < 3.0 NSUV During-RT < 3.0 NSUV During-RT > 3.0 NSUV During-RT > 3.0 NSUV=tumor SUVmax/Aorta SUVmean. (Kong et al, ASTRO 2009)
Proposed RTOG/ACRIN Trial • Followup to ACRIN 6668/RTOG 0235. • FDG-PET during RT • Validate UM results • Study adaptive RT/dose escalation • Randomization to assess the efficacy of mid-treatment FDG-PET • Opportunity to study a novel tracer (e.g. F-Miso) in limited institution sub-study.
RTOG 1106/ACRINxxxx RTOG 0617 arm: Standard dose script Study arm: Individualadaptive RT Estimated Sample size: ~120 patients (85% power to detect 20% difference in 2-yr. local PFS)
Secondary Aims • To compare toxicity between such a PET image-guided adaptive dose escalation and conventional RT. • To validate recent findings from a single institution that a tumor metabolic response during-RT predicts long term local tumor control, LPFS and overall survival. • To perform a pilot study to assess whether a novel PET tracer (F-Miso) is more predictive than FDG-PET. • To obtain blood and tissue samples to explore relationships between imaging findings, biomarkers and outcomes (both anti-tumor efficacy and toxicity).
FLT versus F-Miso Which is the ‘better’ exploratory agent?
Other Issues Still to be Resolved • ACRIN Co-PI TBA. • Radiotherapy Fractionation issues. • Randomization, stratification issues. • Sample size for FLT/FMISO sub-study. • Insurance company reimbursement for mid course PET.