Download
1 / 39
390 likes | 545 Vues
Documenting Disability for Medi-Cal and Social Security. Joe Hennen Vocational Rehabilitation Services Chris A. Douglas Legal Aid Society of San Mateo County. Outline of Training. Primer of Disability Benefits SSI and SSDI Medi-Cal and Medicare Application Process

E N D
Documenting Disability for Medi-Cal and Social Security Joe Hennen Vocational Rehabilitation Services Chris A. Douglas Legal Aid Society of San Mateo County
Outline of Training • Primer of Disability Benefits • SSI and SSDI • Medi-Cal and Medicare • Application Process • Definition of Disability & Proving It • Special Issue: Alcohol and/or Drugs • Group Discussion • Issues/Questions/Comments • San Mateo County Resources 2
Social Security Primer SSA administers 2 disability programs: • SSI – Supplemental Security Income • Cash assistance payments to disabled, blind, and elderly individuals who have limited income and resources. • The federal government funds SSI through general tax revenues and California supplements the federal rate. • Automatically receive Medi-Cal. • SSDI – Social Security Disability Insurance • Monthly disability benefits based on an insured worker's earnings. Need to have worked enough to be covered. (SS Trust Fund) • No income or resource limits attached to SSDI benefits. • Beneficiary receives Medicare in 24 months. • Both programs have different and complicated rules
Social Security Programs Social Security Disability Insurance (SSDI) • a.k.a. Title II, SSA, DIB, RSDI • Insurance program–work credits • Amount based on work history • No Means Test • No Resource Test • Blind or Disabled • Link to Medicare Supplemental Security Income (SSI) • a.k.a. Title XVI, SSI/SSP • In CA $845/mo. for most adults • Reduced if other income, deeming or in-kind support • Low Income, Low Resources (<$2,000 for individual, $3,000 for couple) • U.S. resident and citizenship or qualified immigration category (otherwise CAPI) • Aged, Blind or Disabled • Link to Medi-Cal
Health Care Coverage • Medicare – 65 & older or 24 months on SSDI • Parts A, B, C and/or D • Can have premiums, co-pays, deductibles and coverage gaps • If income/resources are low, may also apply through County for Aged/Disabled Medi-Cal • Medi-Cal—California’s Medicaid • Automatic with SSI, no waiting period • May apply with County if not on SSI • Many different ways to link to Medi-Cal • Free or Share of cost (SOC) • CA Working Disabled Medi-Cal (250%) program
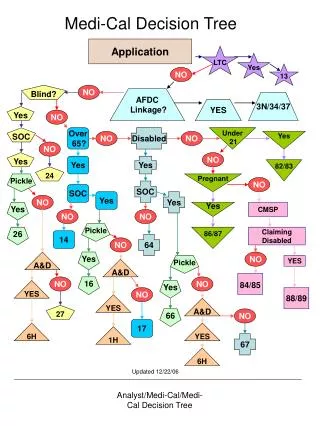
Call SSA at 1-800-772-1213 or file claim online to establish Protective Filing Date SSI Application Process Overview Complete Application and Disability Report SSA Determines Non-Medical Eligibility SSA Sends Medical Information & Releases to State DDS, Where A Disability Analyst Is Assigned DDS Processes & Makes Disability Determination Claimant’s Folder Is Returned To Local SSA Office SSA Notifies Claimant of Decision By Letter 7
SSI Application Process-DDS • Disability Determination Service • State agency with Social Services • Analyst requests & reviews medical records • Medical Consultant review medical records • Decision based on paper file • Might not get all existing medical records • Do not see or examine claimant directly • May Send to Consultative Exam (CE) with a non-treating clinician 8
Establishing Disability • SSA’s Definition of Disability & Proving It • 5-step sequential evaluation process • A closer look at functional limitations and residual functional capacity • Special Issue-Drug Addiction & Alcoholism • Your Role in Documenting the Disability • What SSA/DDS considers • Assembling a Good Application • The Medical Source Letter
Social Security’s Definition of Disability (for Adults) “The inability to do any substantial gainful activity by reason of any medically determinable physical or mental impairment which has lasted or can be expected to last for a continuous period of not less than 12 months or result in death.” • SGA in 2011 is $1000. Or working 30 hours per week earning minimum wage of $8.00. 13
Is the claimant engaged in substantial gainful activity? If yes, not disabled. If no, proceed to step 2. Does the claimant have a severe impairment? If no, not disabled. If yes, proceed to step 3. Does the claimant have an impairment that meets or equals a listed impairment? If yes, disabled. Process stops, you win! If no, proceed to step 4. Can the claimant return to his or her past relevant work? If yes, not disabled. If no, proceed to step 5. Can the individual do any type of work that exists in significant numbers in the national economy? If yes, not disabled. If no, disabled. You win! 5-Step Disability Evaluation Process 1. 2. 3. 4. 5.
Disability--Steps 1 & 2 • Step One: SGA—Is the Person Working? • Engaged in Substantial Gainful Activity (SGA) (~$1,000/mo. for a disabled individual) • Substantial and Gainful • Step Two –Is the Impairment Severe? • Significantly limits an individual’s physical or mental abilities to do basic work activities • Need only show more than minimal limitation • Low threshold to proceed to step 3 15
Step 3: The Listings • Examples of Conditions That are Presumed to Be Disabling • Compare Diagnosis, Symptoms, Clinical Findings, and Functional Limitations to the Criteria of the Listings • If Medical Records Show Claimant’s Condition Meets or Equals A Listing, Then Patient Should be Found Disabled • Organized Into 14 Body Systems 16
Drug Addiction & Alcoholism • SSA no Longer Considers Drug addiction or alcoholism (DA&A) alone to be disabling • If there is evidence of DA&A, must show that impairments would still meet a listing disability criteria without DA&A • An individual does not need to be clean and sober to qualify 17
Substance Addiction Disorders 12.09 Behavioral or physical changes associated with regular substance use that affects the central nervous system. The required level of severity is met when the requirements of any of the following (A through I) are satisfied: A. Organic mental disorders - 12.02 B. Depressive syndrome – 12.04 C. Anxiety disorders – 12.06 D. Personality disorders – 12.08 E. Peripheral neuropathies – 11.14 F. Liver damage – 5.05 G. Gastritis – 5.00 H. Pancreatitis – 5.08 I. Seizures – 11.02 or 11.03 18
Drug Addiction & Alcoholism • Need to identify other physical and/or mental impairment(s) • Tip: Ask claimant whether the reported problems occur when s/he is sober or only when using. • Document functional impairments that exist when sober. • If active use: comprehensive history exploring onset of impairments, trauma, abuse, foster care, education, emotional and physical health. 19
Affective disorders (Step 3) – Mental 12.04(B) • 12.04 Affective disorders: Characterized by a disturbance of mood, accompanied by a full or partial manic or depressive syndrome. Mood refers to a prolonged emotion that colors the whole psychic life; it generally involves either depression or elation. The required level of severity for these disorders is met when the requirements in both A and B are satisfied, or when the requirements in C are satisfied. A. Medically documented persistence, either continuous or intermittent, of one of the following: 1.Depressive syndrome characterized by at least four of the following: • a. Anhedonia or pervasive loss of interest in almost all activities; or b. Appetite disturbance with change in weight; or c. Sleep disturbance; or d. Psychomotor agitation or retardation; or e. Decreased energy, or f. Feelings of guilt or worthlessness; or g. Difficulty concentrating or thinking; or h. Thoughts of suicide; or i. Hallucinations, delusions, or paranoid thinking; or [manic or bipolar syndrome]
Sample Listing (Step 3) – Mental, 12.04(B), (C) B.Resulting in at least two of the following: 1. Marked restriction of activities of daily living; or 2. Marked difficulties in maintaining social functioning; or 3. Marked difficulties in maintaining concentration, persistence, or pace; or 4. Repeated episodes of decompensation, each of extended duration; or C. Medically documented history of a chronic affective disorder of at least 2 years’ duration that has caused more than a minimal limitation of ability to basic work activities, with symptoms and signs currently attenuated by medications or psychological support, and one of the following: 1. Repeated episodes of de-compensation, each of the extended duration; or 2. A residual disease process that has resulted in such marginal adjustment that even a minimal increase in mental demands or change in the environment would be predicted to cause the individual to decompensate; or 3. Current history of 1 or more years’ inability to function outside a highly supportive living arrangement, with an indication of continued need for such an arrangement.
Medical Equivalency (Step 3) – Meets or Equals a Listing • Equals a Listing: Do Not Have Required Specific Clinical Criteria to Meet Listing • but functional limitation of impairment is as severe as a listed impairment • Could be Combination of Impairments: • Several impairments, none of which meets or equals a listing by itself • Combined effect, including effects of obesity, creates functional limitations equal to that of a listing 22
Step 4: Ability to Work • Can the Claimant Return to His or Her Past Relevant Work? • based on Residual Functional Capacity • Past Relevant Work = Substantial Gainful Activity within past 15 years • If Yes, Not Disabled (Ends Here) • If no--go to Step 5 23
Step 5: Ability to Work • Able to Do Any Work That Exists in Significant Numbers in the National Economy Despite Limitations? • Use “Grids” to show not disabled • Any job - need not be actually available • If Yes (can do a hypothetical job), Not Disabled • If No, Disabled 24
Understanding, Remembering, and Carrying Out Simple Instructions Making Simple Work-Related Decisions Responding Appropriately to the ordinary stress of a work-day or work-week Interacting Appropriately with Supervisors, Co-workers, or the public Keeping Regular Attendance Dealing with Changes Can Patients Meet the Basic Mental Demands of Work?
RFC: Activities of Daily Living • Do They Need Help with Basic Activities of Daily Living? • Do They Have Difficulty Caring for: • Self: taking medications, grooming and hygiene • Home: shopping, cooking, cleaning • Finances: paying bills, managing money • Moving Through the World: • Using telephone, public transit, driving 26
Proving Disability Medical Documentation • Medical Records Are Needed to Document Impairment(s) • Treating Source Should be Given Most Weight (Treatment Team) • If consistent with record • Longer relationship = more weight • Examining > Non-Examining • Specialists> Non-Specialists 27
Medical Documentation & Proof • M.D. or Ph.D. Opinion is Given Most Weight (can sign off as supervisor of a treatment team) • Other Sources are Entitled to Some Weight (hierarchy of evidence): • M.D. or Ph.D. > other clinicians (e.g., MFT, LCWS, RN, NP) • Lay witnesses (teachers, relatives, etc.) • Claimant’s subjective complaints 28
Non–Medical Sources • Lay Witnesses & Claimant • Non-Medical Sources Can Elaborate on Severity of Impairment • Effects on Daily Activities, Exertional; and Non-Exertional Limitations. • Statements from Claimant and Third-Parties can Bolster Underlying Medical Evidence 29
The Clinician’s Role • Document disability • Cite to objective evidence • Describe functional limitations • Do not need to draw conclusion regarding ability to work • DDS/SSA’s role is to decide if a Patient is disabled – the clinician’s role is to document 30
Documenting the Impairment • DDS Must Consider Combination of Mental and or Physical Impairments, and Resulting Functional Limitations • Consider Interaction of Impairments • e.g., Depression and Chronic Pain or Depression and Heart Disease • Condition Exacerbated by Obesity? • Side Effects of Medication 31
Narrative Summaries • Medical Source Statements and Letters Increase Success Rates • Review the Listings • compare clinical findings, symptoms, etc. • Do not need to conclude if listing met, but include any relevant evidence • Include Details, not just conclusions • Describe severity, duration, include all relevant details and functional limitations 32
Pulling It All Together: A Good Disability Application • Gather & Submit Medical Records • Physical & mental health records • School / special education records • Refer for other treatment if needed • Gather Social & Work History • Provide a Current Assessment or Medical Source Statement • Include any Third Party Reports 33
Top factors in determining who to encourage and who to help to apply • Patient’s financial situation • Diagnosis • Current functioning • Prognosis • Co-occuring AOD issues • Work history
The Recovery Model • Economic and food insecurity are impediments to recovery. • All public benefit programs have work incentives to get people off benefits. • The entire system benefits from having all eligible individuals receiving public benefits.
SSI and SSDI “Employment Supports” • Once on benefits there are special rules that allow a person to work and: • Continue to receive monthly cash benefits • Have benefits restart if substantial work stops • Keep Medicare or Medi-Cal • Help with training and special expenses • Separate Rules forSSDI andSSI programs
Group Discussion • Deciding who to help: • Who are the best candidates • How do we identify them • How do we help: • Who to contact • How to support the client • How to get documentation • Does helping clients apply fit our philosophy? • Limiting individuals recovery 38
Disability Benefits Planning & Assistance Resources • VRS Financial Empowerment Project (FEP) 550 Quarry Road, San Carlos, CA (650) 802-6578; 802-6486 • Center for Independence of Disabled (CID) 1515 S. El Camino, CA 94402 (650) 645-1780 • Legal Aid Society of San Mateo – Mental Health SSA Project 5th Ave, San Mateo, CA 94402 (650) 558-0915 • San Mateo County Medi-Cal TeleCenter 1-800-223-8383 • HICAP, The Medicare Counseling Program 1-800- 434-0222 • DB101.org website