Download
1 / 41
410 likes | 622 Vues
Alzheimer’s Disease for Emergency Personnel. Helle Brand, PA Banner Alzheimer’s Institute. Objectives . Describe Alzheimer’s disease Outline the impact of coexisting diseases on dementia and discuss delirium Identify the challenges of providing care to patients with dementia

E N D
Alzheimer’s Disease for Emergency Personnel Helle Brand, PA Banner Alzheimer’s Institute
Objectives Describe Alzheimer’s disease Outline the impact of coexisting diseases on dementia and discuss delirium Identify the challenges of providing care to patients with dementia Discuss specific strategies to enhance care and outcomes for patients with dementia
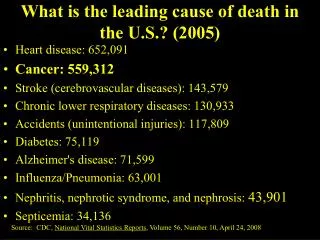
Demographics of Dementia 5.3 million Americans have dementia By 2050, numbers will more than triple About 10% of age 65+; nearly half of those 85+ are affected Average life expectancy following diagnosis is 8 – 10 years 6th leading cause of death among older Americans
About Dementia… • Dementia is not a specific diagnosis • Each type of dementia has unique features and is progressive • Most common types of dementia include: • Alzheimer’s disease (AD) • Lewy body dementia (LWD) • Vascular dementia (VaD) • Frontotemporal dementia (FTD)
I N D E P E N D E N C E T I M E Progression of Dementia Reference: Hurley & Volicer, 1998
Function Cognition Behavior Clinical Presentation of Dementia
Insidious onset with progressive decline • Impaired social or occupational functioning • Memory loss • Cognitive loss in at least 1 other domain • Language • Calculations • Orientation • Judgment • Deficits not due to other systemic disease • Deficits NOT in the setting of a delirium DSM IV Criteria for Alzheimer’s Dementia
Early (MILD) Stage Features • Short term memory loss • Problems with language and abstract thinking • Misplacing things • Disorientation of time • Poor/ decreased judgment • Changes in mood/behavior and/or personality • Loss of initiative • May have difficulty in a crowd Treatment • Cholinesterase Inhibitor • Manage depression and other co-existing health problems Maintaining Independence
may get lost driving or be unsure of self in new surroundings • Forget appointments, family events • Lists may not make sense • May compensate for weaknesses • GRADUAL DECLINE IADLs Early changes in AD, continued
Medication management • Driving • Weight loss • Mood, especially depression • Changing awareness and concern for safety • Need for life planning: financial, legal • Balancing autonomy vs supervision Special concerns early on
Memory loss, confusion and attention worsen over a 2-10 year span • Judgment and problem solving a problem Can’t think logically, organize thoughts Loss of ability to handle complex tasks and technology, gradual problems with taking care of self • Personality and behavior changes • Increasing dependence • Increasing language difficulties • Vulnerable adults, cannot live alone Moderate Stage Alzheimer’s
Middle (MODERATE) Stage . Living with help
Behaviors: suspiciousness, irritability, restless, impulsivity, seeing or hearing things not present, agitation, wandering, sleep disturbance, disinhibition • Changing communication/expectations • Increasing dependence, behaviors cause increasing caregiver burden/stress • Safety: need 24 hour supervision • Recognizing delirium Concerns with mid stage AD
Memory loss is severe, including long term • Loss of recognition of others beyond self • Problems controlling bowel/bladder • Fully dependent for care needs • Minimal to no speech • Changes in posture/walking, may not walk and/or become bed bound • Neurologic changes: myoclonic jerks, seizures, dysphagia Late to End Stage Alzheimer’s
Risk for falls • May be prone to infection or skin breakdown • Weight loss • Potential for seizures • Increasing sleep • Planning for death and dying • Comfort in terms of mood and pain • TIMELY HOSPICE REFERRAL Issues in advanced Alzheimer’s
Dementia + Comorbidities • Large numbers have chronic medical issues • Acute medical issues associated with advanced dementia • Medications can hasten decline • Antihistamine, anticholinergics, corticosteroids, anti-parkinson, hypnotics, sedatives, opioids, ETOH Maslow, NurCl N Am, 2004; 39: 561-579; Feil et al. JAGS 2007; 55:S293-301.
Those with some form of dementia are at increased risk for developing delirium • Delirium is a risk factor for future delirium and for developing a permanent dementia • Age contributes to both • Medications play a role • Recognition of symptoms and treatment is critical What we need to know about delirium and dementia
At least 25% >70 are admitted with delirium • Occurs in about half of elderly patients during or after acute hospitalization • More than half of these are found to have permanent dementia, previously undiagnosed • Up to 70% of ICU patients develop delirium • Delirium occurs in 28 – 83% of patients near the end of life (terminal agitation, restlessness) Incidence of Delirium Girad, Crit Care. 2008;12 Suppl 3:S3. Epub 2008 May 14; Waszynski, AJN, 2007, 107:12, 50-59
D: dementia • E: electrolytes, dehydration • L: lung, liver, heart, kidney, brain • I: infection • R: Rx drugs • I: injury/pain/stress • U: unfamiliar environment • M: metabolic Causes of Delirium
Delirium Abrupt onset (hours – days) Duration days to weeks Symptoms include confusion, forgetfulness, altered sleep-wake cycle, high frequency of delusions, hallucinations and illusions Causes include acute medical conditions, meds, ETOH abuse, acute psychosis Treatment of underlying condition; supportive techniques Dementia Insidious onset (months – years) Duration 2-20 years Symptoms include decline in memory, speech/ language difficulty, loss of self-care abilities and a variety of behavior problems Causesdepends of etiology of disease Treatment limited to managing symptoms and behaviors In summary, how to differentiate Delirium vs. Dementia
Your challenges with confused patient Assessing confusion: Delirium v. Dementia or Delirium Superimposed on Dementia Safety Identification and treatment of pain Health Care Decisions Family Caregivers
Confusion Assessment Method • Feature 1: Acute Onset or Fluctuating Course • Is there any evidence of an acute ∆ in MS from baseline? Did the behavior fluctuate during the day, increase/decrease in severity? • Feature 2: Inattention • Did the patient have difficulty focusing attention, being easily distracted, or have difficulty tracking conversation? • Feature 3: Disorganized thinking • Was the patient’s thinking disorganized or incoherent, unclear, rambling or switching topics? • Feature 4: Altered Level of Consciousness • Overall, how would you rate the patient’s level of consciousness? Alert - Vigilant – Lethargic – Stupor - Coma Inouye, S. (1990) Annals of Internal Med 113(12) 941-948.
Clock Drawing • Simple screening tool: • Ask the patient to draw a clock • Place all the numbers on the clock • Set the time at 11:10 • Scoring: 5 points totals • 1 point for the clock circle • 1 point for the numbers in correct order • 1 point for numbers being in proper special order • 1 point for two hands of the clock • 1 point for the correct time
1. What are the date, month, and year? 2. What is the day of the week? 3. What is the name of this place? 4. What is your phone number? 5. How old are you? 6. When were you born? 7. Who is the current president? 8. Who was the president before him? 9. What was your mother's maiden name? 10. Can you count backward from 20 by 3's? SCORING:* 0-2 errors: normal mental functioning3-4 errors: mild cognitive impairment5-7 errors: moderate cognitive impairment8 or more errors: severe cognitive impairment*One more error is allowed in the scoring if a patient has had a grade school education or less.*One less error is allowed if the patient has had education beyond the high school level. SPMSQ
Describe actual behaviors or symptoms demonstrated and the frequency which they occur • Determine if the behavior is new or has increased in frequency • Obtain from family any successful interventions for identified behaviors Assessment of Behavior(s)
Moderate Dementia: Resisting/fighting hands-on caregivers Assaultive toward caregivers/peers Wandering and rummaging Physical restlessness Sundowning Eating problems Sleeping problems Yelling Sexual behaviors Advanced Dementia: Resisting/fighting hands-on caregivers Fall risk (wanting to walk when unable to) Physical restlessness Resisting/refusing to eat/drink Disruptive sleep patterns Disruptive yelling Common behaviors
Decreased ability to recognize familiar places and faces • Can forget names, addresses • Become disoriented • Decreased reasoning and judgment • Behavioral changes • Increasing confusion • All worse with any stressors • concrete thinking Let’s remember!
Introduce yourself at each encounter • Use touch as appropriate • Start with the “Soft Approach” • Smile, warm demeanor • Remain calm, reassuring, RESPECTFUL • Pleasant voice and tones • Go slow • Talk in short, simple sentences; rephrase • Avoid correcting/confrontation • aka CONNECT NOT CORRECT • Actions help when communication may fail: use gestures, demonstrate, touch affected areas Approach Strategies
Anticipate and meet basic comfort needs such as continence care, food/fluids, positioning, room temperature • Give the patient something to hold on to such as a washcloth, stuffed animal, doll, your hand, etc. • Food is ultimate distractor • Touch • Sing or play music • Read a prayer, poem, scripture verse Comfort Techniques
Antipsychotics to manage psychosis (delusions, paranoia, hallucinations) • Mood stabilizers (for aggression/mania) • Trazadone for sleep • Avoid benzodiazepines to manage psychosis or agitation • Avoid medications with anticholinergic properties Pharmacological Interventions
Maintaining Safety • Falls due to impulsivity, confusion • Compliance with care, may pull at tubes, resist medications • Psychosis: hallucinations, misperceptions, paranoia, delusions • Home situation: weapons
Identification & Treatment of Pain Patients with moderate to severe dementia cannot reliably report pain Pain is often under recognized and under treated in dementia patients Pain tolerance does NOT change due to dementia Pain left untreated will lead to challenging behaviors such as striking out and yelling
0 1 2 Score Breathing Independent of vocalization Normal Occasional labored breathing. Short period of hyperventilation. Noisy labored breathing. Long period of hyperventilation. Cheyne-stokes respirations. Negative Vocalization None Occasional moan or groan. Low level speech with a negative or disapproving quality. Repeated troubled calling out. Loud moaning or groaning. Crying. Facial Expression Smiling, or inexpressive. Sad. Frightened. Frown. Facial grimacing. Body Language Relaxed. Tense. Distressed pacing. Fidgeting. Rigid. Fists clenched, knees pulled up. Pulling or pushing away. Striking out. Consolability No need to console. Distracted or reassured by voice or touch. Unable to console, distract or reassure. How to Measure Pain? PAINAD Warden et al. J Am Med Dir Assoc 2003, 4: 9-15.
Pharmacological Interventions for Pain Routine administration of acetaminophen up to 3 grams daily for mild to moderate pain Use small doses of opioids for moderate to severe pain If pain medications are effective, they should be ordered routinely NOT prn Use other strategies as well!
Use the family as appropriate: identify baseline, changes; effective strategies • Medic Alert bracelets: • Other technologies: GPS, radio transmitters for repeat wanderers • Community education Other considerations