Download
1 / 27
270 likes | 277 Vues
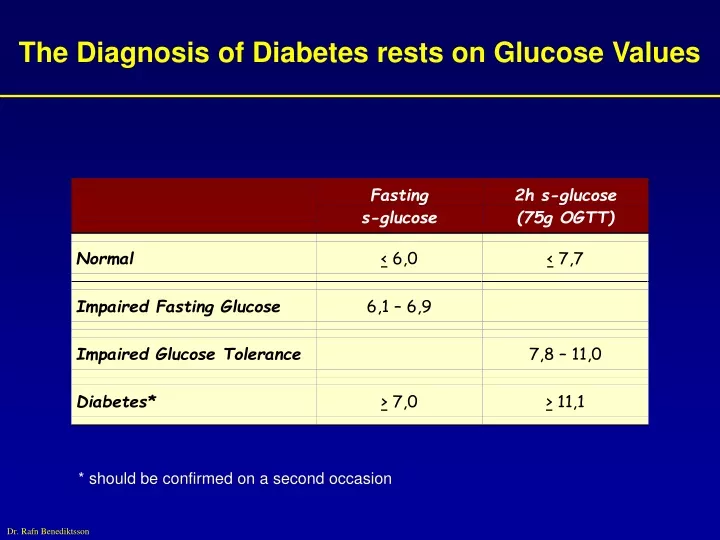
The Diagnosis of Diabetes rests on Glucose Values. * should be confirmed on a second occasion. Type 2 Diabetes: Development. Insulin resistance. Impaired -cell function. Insulin resistance and hyperinsulinaemia with normal glucose tolerance.

E N D
The Diagnosis of Diabetes rests on Glucose Values * should be confirmed on a second occasion
Type 2 Diabetes: Development Insulin resistance Impaired -cell function Insulin resistance and hyperinsulinaemia withnormal glucose tolerance Insulin resistance and declining insulin levels with impaired glucose tolerance Type 2 Diabetes Adapted from Saltiel AR, Olefsky JM. Diabetes 1996;45:1661-1669.
What is Insulin Resistance? An impaired biological response to either exogenous or endogenous insulin Biological responses could reflect: metabolic(CHO, lipid or protein metabolism) and mitogenicprocesses (changes in growth, differentiation, DNA synthesis, regulation of gene transcription) Anonymous. Diabetes Care 1998; 21:310-314.
Insulin Resistance: Associated Conditions Type 2 diabetes Impairedglucose tolerance Atherosclerosis Dyslipidaemia Hypertension Insulin Resistance Decreasedfibrinolytic activity Obesity (central) Polycysticovarian syndrome Microalbuminuria Hyperuricemia
Risk Ratios of CV Events in Adultswith Diabetes Age 35-64 † † 9.8 9.1 † 6.1 † † † 4 † 3.9 Risk Ratio † 3 2.8 2.8 * 1.8 1.9 † p <0.001 *p < 0.05 Adapted from Wilson & Kannel. In Ruderman et al. Hyperglycaemia, Diabetes and Atherosclerosis 1992:21
Drug Treatment in T2DM Acarbose Reduces absorption Insulin “Replaces” pancreas Carbohydrate DIGESTIVE ENZYMES Glucose I G Glucose (G) Sulphonylurea Repaglinide Stimulates pancreas I I G Insulin G (I) I G G I G I G I G I G Metformin Reduces hepatic glucose output (? muscle / fat effects) I G G
Lowering HbA1C Reduces Risk of Complications* *Percent risk reduction for 0.9% decrease in HbA1C UKPDS. Lancet 1998; 352:837
UKPDS: Value of Good Blood Pressure Control in T2DM risk reduction37% p=0.0092
VA - HIT Study: Effect of Gemfibrozil on Vascular Events - 5.1 Years % of Patients with CHD Death, Nonfatal MI, or Stroke 24% Risk Reduction 40 35 36 24% Risk Reduction 30 % Developing a CV Event 28 25 23 20 18 15 10 5 0 Placebo Gemfibrozil Placebo Gemfibrozil Patients with Diabetes n=627, P=0.05 Patients without Diabetes n=1904, P=0.009 Rubins HB, et al. N Engl J Med 1999;341:410
Drug Treatment in T2DM Acarbose Reduces absorption Insulin “Replaces” pancreas Carbohydrate DIGESTIVE ENZYMES Glucose I Glucose (G) G I Sulphonylurea Repaglinide Stimulates pancreas I G Insulin G I (I) G G I G I G I G I G I Metformin Reduces hepatic glucose output (? muscle / fat effects) G G Thiazolidinediones (TZD)
TZD: Mechanism of Insulin Sensitization INSULIN RECEPTOR Protein –signalling –downstream events TZD PPAR RXR RNA TZD PPAR TF RXR DNA TZD = thiazolidinedione PPAR - RXR = nuclear receptors TF = transcription factors Saltiel & Olefsky. Diabetes 1996;45:1661
Rosiglitazone Enhances Insulin Action by Modulating Tissue Lipid Supply Reduced Hepatic Glucose Output Adipocyte Liver Reversal of TNF-Induced Insulin Resistance GLUT-4 Reduced Lipolysis, Glycerol, & FFAs Availability Increased Insulin Sensitivity and Capacity for Glucose Disposal/Lipid Storage Euglycemia PPAR Rosiglitazone and Insulin Skeletal Muscle PPAR TG Preadipocyte Increased Glucose Disposal Increased Differentiation
Effect of Pioglitazone on Insulin Resistance (HOMA R) 30.3* † Baseline IR: placebo 10.1, pioglitazone 30 mg 9.8 * p = 0.0002 vs baseline † p = 0.0001 vs placebo Rosenstock I, et al. Diabetologia 2000;43(suppl 1):A738
Effect of Pioglitazone on Abdominal Fat Distribution Miyazaki Y et al. Diabetes 2000;49(SI);A299.
TRIPOD: Buchanan et al. Diabetes 2001;50(S2):A327 Placebo for 30 months A 235 Latino women with GDM Troglitazone for 30 months 20 16 B 12 Observ. for 8 mo.: OGTT % with diabetes 8 4 0 Placebo Troglitazone
PCOS: Improvement in hirsutism by troglitazone PBO TGZ150 TGZ300 TGZ600 4 2 0 -2 -4 -6 % change in FG score -8 -10 -12 -14 -16 * -18 -20 Azziz et al JCEM 2001;86:1626
Effect of Pioglitazone on Serum Lipids Effects by Glycaemic Response D from placebo at 26 weeks 20 Glycaemic Non-Responders (45 mg) * * 11.5 Total Cohort (45 mg) 9.5 10 4.6 2.1 1.6 1.2 (%) 0 -10 -13.6 - 15.1 -20 * Triglycerides Total Cholesterol HDL Cholesterol LDL Cholesterol Baseline (mmol/L) 6.27 1.07 1.05 3.29 3.28 2.66 2.93 5.45 LOCF* p£ 0.05 vs. placebo Takeda Pharmaceuticals America, Inc., data on file, study 001
Inflammation: Effect of rosiglitazone on CRP N = 357, treatment for 26 weeks Greenberg et al @ EASD 2001
PPARg activators inhibit migration of VSMC 100 % of migration compared to PDGF-BB 50 0 PDGF - + + + 5 µM 10 µM troglitazone Marx et al.; Circ Res 1998; 83: 1097-1103
Rosiglitazone inhibits the insulin-mediated increase in PAI-1 secretion in human subcutaneous adipocytes CTRL Insulin [nM] Mcternan @ EASD 2001
Nitric oxide synthaase inhibition decreases the increased insulin action by piogllitazone in the fructose–fed rat 3 mU/kg/min insulin iv 12 10 8 Glucose disposal rate [mg/kg/min] 6 4 2 0 STD FRUCT FRUCT FRUCT - - + + PIOGLITAZONE - - - + L-NMMA Koshinaka @ EASD A98
The ischaemic obese Zucker rat heart * Sidell @ EASD 2001
Rosiglitazone reduces atherosclerosis in ApoE KO mice Benson et al @ EASD 2001
potential proatherogenic effects potential antiatherogenic effects ECs ECs MCP-1, IL-8 VCAM-1, endothelin PPARg IL-6, prostaglandin, COX-2 PPAR SMCs SMCs Mo / MØ Mo / MØ Tissue factor, TNF-a apoptosis CXC chemokines, endothelin, PAI-1 ECs ECs PAI-1 migration, MMP-9, Ang-II-receptor SMCs SMCs NO production MMP-9; cytokines, SR A,I-NOS CD 36 Foam cell formation apoptosis Mo / MØ Mo / MØ TH-1 cytokines T-cells
Niðurstaða • Thiazolidinedione lyf eru leyfð á Íslandi sem meðferð við sykursýki • Eingöngu sem viðbót við eitt annað per os blóðsykurlækkandi lyf • TZD lyf ráðast að kjarna málsins – Insúlín viðnám – og þannig á ýmsa áhættuþætti hjarta og æðasjúkdóma • In-vitro rannsóknir og dýratilraunir gefa vísbendingar um að TZD lyf geti hugsanlega tafið nýmyndun og framgang atherosclerosis • Ekki eru til klínískar mannarannsóknir á áhrifum TZD á atherosclerosu eða dánartíðni !