Download
1 / 32
350 likes | 1.14k Vues
ENTEROBACTERIACEAE. Dr. Abdulaziz Alkhattaf. coliforms. Non-spore forming, gram negative bacilli. Facultative anaerobic. Catalase + ve ; Oxidase – ve . Motility ±; some are capsulated . Widely dispersed in nature, yet was found to inhabit the intestine of mammalians.

E N D
ENTEROBACTERIACEAE Dr. Abdulaziz Alkhattaf
coliforms • Non-spore forming, gram negative bacilli. • Facultative anaerobic. • Catalase +ve; Oxidase–ve. • Motility ±; some are capsulated. • Widely dispersed in nature, yet was found to inhabit the intestine of mammalians. • Grow well in ordinary media (blood agar, Mc-conkey agar) aerobically or facultative anaerobic.
Identification • Lactose fermentation: • McConkey agar contains lactose and pH indicator + pink colonies. • CLED agar changes from blue-green to yellow colonies. • Biochemical tests: (a)- Reduce nitrate to nitrite. (b)- Ferment glucose with acid (sometimes gas production). (c)- The use of API 20E biochemical kit tests.
Identification of coliforms • Serological tests: • Based on the somatic (O) antigen and the flagellar antigen (H) for the identification of Salmonella and Shigella species. • Bacteriophage typing (using viruses to identify bacteria). • Bacteriocine typing (pigments produced by bacteria). • Plasmid analysis (extra-chromosomal DNA). • Polypeptide analysis (polyacrylamide gel electrophoresis).
Antigenic structure • Enterobacteria possess variety of heterogeneous antigens: • Somatic/cell wall (O) • Flagella (H) • Capsular (K)
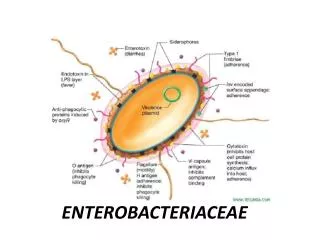
Pathogenicity • Virulence Factors: • Endotoxin: Lipopolysaccharide Lipid A: toxin Polysaccharide: antigenic • Capsule –antiphagocytic. • Pili -for attachment ( K88 of E.coli→dirrhoea/infant pigs) • Enterotoxins→ e.gE.coli causing diarrhoea.
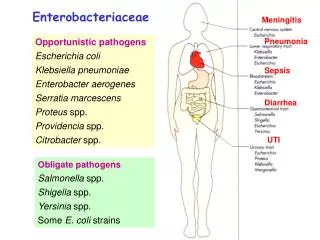
Pathogenicity • Diseases: • Intestinal Salmonella }Primary • Shigella } intestinal Pathogens. • E.coli:some strains are intestinal • Pathogens. • Extra-intestinal • UTI –Coliforms contribute up to 80% UTI. • Wound infections/ post operative. • Respiratory tract infection. • Septicaemia. • Meningitis→neonates (E.coli) /or with trauma /surgery
Antibiotic sensitivity • Enterobacteria are resistant to multiple antibiotics. • In vitro sensitivity testing is required to monitor the trend and to assess based on case by case. • The most common antibiotic used are: • Ampicillin/ amoxycillin and mezlocillin. • Aminoglycosides. • Trimethoprim. • Chloramphenicol. • Ciprofloxacin. • Cephalosporins (2nd,3rd generations) • Nitrofurantoin, Nalidixic acid/ UTI only.
Escherichia coli • Serology of E.coli: • According to the cell wall (O antigen) over 160 types recognized. • According to the flagellar (H antigen) 55 types. • Making over 8000 possible O-H seotypes. • Some E.coli types are capsulated
Pathogenicity of E.coli • Intestinal:
Pathogenicity of E.coli • Extra-intestinal • Urinary tract infection (UTI)/ causes 80% of UTI in pregnant females. • Wound infection/ Surgery of lower intestinal tract. • Peritonitis. • Septicemia. • Neonatal meningitis.
KLEBSIELLA l ENTEROBACTER/ SERRATIA • Widely spread in the environment/ in the intestine flora of man and animals. • Survive well in moist environments in hospitals. • Opportunistic pathogens → chances of infection are increased in long term hospitalization, ICU. • Grow well on all media /producing large and mucoid colonies (capsule). • Β-lactamases producing/ resistant to ampicillin,1st and 2nd generation of cephalosporins→ therefore we resort to using Aminoglycosides.
Pathogenicity • Urinary tract infection (chronic, complicated infections). • Wounds, skin lesions and respiratory infections in hospitalised patients. • Septicemia. • Abscesses, endocarditis, chronic nasal and oropharyngeal sepsis. • Meningitis (neonates).
PROTEUS /MORGANELLA / PROVIDENCIA • Habitat: Human and animal intestine//soil/ water. • Isolation: Grow well on ordinary media in a swarming type, which cover the plate. • Identification: Swarming, and all species produce a potent urease enzyme. • phage, bacteriocine and serotyping schemes have been developed for identification there species.
Pathogenesis • Urinary tract infection / urea is split by the Proteus urease to produce ammonia→alkaline urinary pH. • Urease-producing organisms (proteus) may provoke the formation of calculi (stones) in urinary tract. • Ear ,wound and burn infections (mixed infection). • Septicaemia and brain abcesses.
PSEUDOMONAS • Gram Negative Bacilli; non-fermentative strictly aerobic, motile and oxidase positive. • Pseudomonas species commonly inhibit soil, water and are widely spread. Can use variety of carbon and nitrogen sources. • Difficult to eradicate / especially in hospital wards, operating theatres and medical equipments (respiratory ventilators) being resistant to many disinfectants. • clinical isolates produce a characteristic green or blue-green pigment called Pyocyanin. Also produce Pyoverdin(fluorescein) a yellow-green pigment↔fluoresces under UV light .
Pathogenesis • Ps.aeruginosa is an important opportunistic pathogen. • causing infection in immunocompromised patients / burns, HIV,cancer and cystic fibrosis patients. • pseudomonas enters blood stream causing sepsis with 50% mortality rate. • spread to skin causing black necrotic lesions (ecthymagangrenosum). • Severe external otitis (malignant otitisexterna). • other skin lesions (folliculitis)↔ inadequate chlorinated swimming pool users. • Corneal infections↔ contact lens users.
Treatment • Psedomonas is resistant to many antibiotics /e.g penicillin, ampicillin, tetracycline, most cephalosporins. • Psedomonas infections were usually treated with polymyxins, now stopped for its high toxicity. • Antipseudomonalβ-lactam compounds such as zlocillin, ticarcillin, imipenem and ceftazidime are commonly used. • Aminoglycosides such as gentamicin and tobramycin are also used and some times with combination β-lactams. • Fluoroquinolones (ciprofloxacin) can be given orally.
Epidemiology • Species have the ability to multiply on moist equipments (humidifiers) in hospital wards, bathrooms& kitchens. • Resistant to many disinfectants and antiseptics. • Can contaminate pharmaceutical preparations and may cause ophthalmitis to contact lenses users. • Important cause of nosocomial infections 10-30% of hospital-acquired infections. • Airborne pseudomonas is hazardous to burned and ICU patients. • Ear infection and irritating folliculitis (jacuzzi rash) occur due to poorly maintained swimming pools or jacuzzis.
Pseudomonal control • Prevention is easier than cure: • Immunocompromised and patient with high risk of acquiring Ps. aeruginosa should not be admitted to a ward with cases of such infection are present. • Therapeutic substances must be free from Ps especially multi-dose ointments, creams or eye drops. • Using typing system to identify cross-infection of one strain (epidemic strains).
Acinetobacter • Gram negative coccobacilli resemble Enterobacteriaceae in growth pattern and colonial morphology. • Incapable of fermenting carbohydrates or reduce nitrates. • Appear frequently as skin and respiratory colonizers. • Frequently contaminate wet objects including soaps and disinfectant solutions. • Pneumonia, urinary tract and soft tissue are the most common infections
Nosocomial respiratory infections are traced to contaminated inhalation therapy equipments whereas bacteremia to infected intravenous catheters. • Due to frequent resistance to penicillins, cephalosprins and some aminoglycosides treatment is difficult and required prior sensitivity testing.
Moraxella • Gram negative coccobacilli in pairs. • Fastidious growth (required enriched media-chocolate agar). • Due to similarity in morphology and positive oxidase reaction Moraxella is some times confused with Neisseria. • Causes otitis media, sinusitis and lower respiratory infection.
Burkholderiapseudomallei • Free living saprophyte that causes melioidosis, a devastating tropical infection of animal and humans that is endemic in eastern Asia and north Australia. • Laboratory-acquired infection is a serious risk; the species is included in hazard group 3 (together with plague).
Melioidosis: • Human infection is mainly acquired cutaneously through skin abrasions or by inhalation of contaminated particles. • Clinical manifestation range from a sub-clinical infection, diagnosed by the presence of specific antibodies, to a benign pulmonary infection that may resemble tuberculosis or septicemia with mortality rate of 80-90%. • In north eastern Thailand, B.pseudomallieis responsible for 20% of all community acquired septicemia.
Early diagnosis and appropriate antibiotic therapy are key factors in the successful management of melioidosis. • Organism may be isolated from sputum, urine, pus or blood (gram –ve bacilli). • ELISA is used for detection of IgGanfIgMantibodiy to B.pseudomallieas well as indirect haemagglutination test.
Treatment • Combination of tetracycline and chloramphenicol for long period of time, have been widely used. • The ability of B.pseudomallie to survive and multiply in phagocytic macrophages may explain the difficulty to treat the disease. • Antibiotics that are effective against the organism in vitro are not successful in vivo unless with prolong period of treatment. • Ceftazidime is both effective in vitro and in vivo.
Burkholderiacepacia • Major opportunistic cause of respiratory infection in patients with chronic granulomatous (cystic fibrosis) disease. • The organism is multi-resistance to many antibiotics and transport by social contact. • Cepacia syndrome, an acute fatal necrotizing pneumonia, some times accompanied by bacteraemia is a risk with B.cepacia. • For treatment of B.cepaciaceftazidime or cabapenem, meropenem.
Eikenellacorrodens • Commensal of mucosal surface may cause range of infections such as endocarditis, meningitis, pneumonia and infections of wounds and various soft tissues.
Flavobacteriummeningosepticum • Meningitis with F.meningosepticum is responsible for high mortality in epidemic outbreaks. • Is a saprophyte that could cause opportunistic nosocomial infections in infants.