Download
1 / 36
480 likes | 813 Vues
Inpatient Coding Strategies. American College of Physicians March 1, 2013. Jaci Johnson CPC,CPMA,CEMC,CPC-H,CPC-I. President, Practice Integrity, LLC jaci@practiceintegrity.com. Disclaimer.

E N D
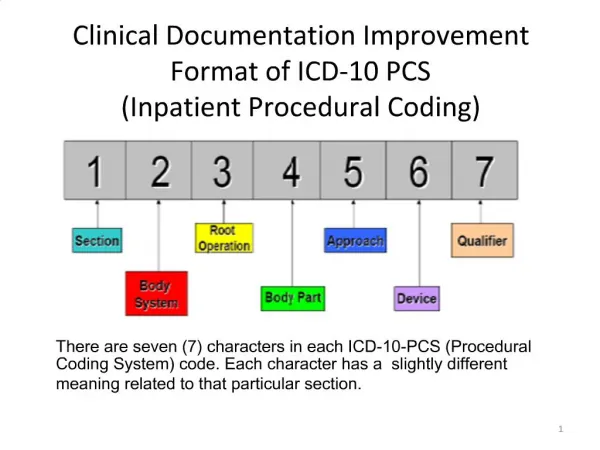
Inpatient Coding Strategies American College of Physicians March 1, 2013
Jaci JohnsonCPC,CPMA,CEMC,CPC-H,CPC-I President, Practice Integrity, LLC jaci@practiceintegrity.com
Disclaimer Information contained in this text is based on CPT®, ICD-9-CM and HCPCS rules and regulations. However, application of the information in this text does not guarantee claims payment. Payers’ interpretation may vary from those found in this text. Please note that the law, applicable regulations, payer’ instructions, interpretations, enforcement, etc., may change at any time. Therefore, it is crucial to stay current with all local and national regulations and policies.
Evaluation and Management READ THE GUIDELINES – Medicare Documentation Guidelines GENERAL PRINCIPLES OF MEDICAL RECORD DOCUMENTATION The principles of documentation listed below are applicable to all types of medical and surgical services in all settings. For Evaluation and Management (E/M) services, the nature and amount of physician work and documentation varies by • type of service, place of service and the patient's status. The general principles listed below may be modified to account for these variable circumstances in providing E/M services.
Evaluation and Management READ THE GUIDELINES – Medicare Documentation Guidelines • The medical record should be complete and legible. • The documentation of each patient encounter should include: • reason for the encounter and relevant history, physical examination • findings and prior diagnostic test results; • assessment, clinical impression or diagnosis; • plan for care; and • date and legible identity of the observer.
Evaluation and Management READ THE GUIDELINES – Medicare Documentation Guidelines • If not documented, the rationale for ordering diagnostic and other ancillary services should be easily inferred. • Past and present diagnoses should be accessible to the treating and/or consulting physician. • Appropriate health risk factors should be identified.
Evaluation and Management READ THE GUIDELINES – Medicare Documentation Guidelines 6.The patient's progress, response to and changes in treatment, and revision of diagnosis should be documented. 7. The CPT and ICD-9-CM codes reported on the health insurance claim form or billing statement should be supported by the documentation in the medical record.
Evaluation and Management READ THE GUIDELINES – Medicare Documentation Guidelines 8. The ROS and/or PFSH may be recorded by ancillary staff or on a form completed by the patient. To document that the physician reviewed the information, there must be a notation supplementing or confirming the information recorded by others.
Evaluation and Management READ THE GUIDELINES – OIG Compliance Policy for Physician Practices Medical Record Documentation. In addition to facilitating high quality patient care, a properly documented medical record verifies and documents precisely what services were actually provided. The medical record may be used to validate: (a) The site of the service; (b) the appropriateness of the services provided; (c) the accuracy of the billing; and (d) the identity of the care giver (service provider).
Evaluation and Management ServicesCredit for Work Done • Coding Based on Time Unit/floor Time If over 50% of the floor/unit time is spent in counseling and coordination of care then time may be used as the indicator for the code selection. Hospital observation, inpatient hospital, inpatient consultations, nursing facility NOT DOCUMENTED NOT DONE
Evaluation and Management Services Hospital Services Choosing the correct level of service is important in hospital setting also.
Hospital Charges • How are they tracked/followed? • Does the diagnosis tell your part of the story? • Do you provide the patient information from the hospital for your staff.
Evaluation and Management Services Hospital admission (99221 – 99223) • Code selection based on level of service or time • Do not bill for other related E&M services on same date of admission • Describes the first inpatient encounter with the patient.
Evaluation and Management Services 99221 (30 minutes) Detailed or comprehensive history and exam Straightforward or Low level Medical Decision Making 99222 (50 minutes) Comprehensive History and Exam Moderate level Medical Decision Making 99223 (70 minutes) Comprehensive History and Exam High level Medical Decision Making
Subsequent Hospital Visits • 99231, 99232, 99233 • Every note stands alone • Why are you there? • What are you doing? • Time • How is the patient? • Was the patient discharged?
Subsequent Hospital Visits • 99231 • Problem Focused Interval History and Problem Focused Examination • S or L Medical Decision Making • 99232 • Expanded Problem Focused Interval History and Exp Problem Focused Examination • Moderate Complexity Medical Decision Making • 99233 • Detailed Interval History and Detailed Examination • High Complexity Medical Decision Making
Subsequent Hospital Visits • 99231 – 15 minutes • Usually the patient is stable, recovering or improving • 99232 – 25 minutes • Usually the patient is responding inadequately to therapy or has developed a minor complication. • 99233 – 35 minutes • Usually the patient is unstable or has developed a significant complicationor a significant new problem.
Subsequent Hospital Visits Do not play it safe by just using 99231
Subsequent Hospital Visits • 99231 • Medicare allows $32.56 • 99232 • Medicare allows $53.18 • 99233 • Medicare allows $75.61
Subsequent Hospital Visits Example: 100 subsequent hospital visits 80 99231 - $ 2605 10 99232 - $ 532 10 99233 - $ 756 Total: $ 3893
Subsequent Hospital Visits Example: 100 subsequent hospital visits 60 99231 - $ 1954 30 99232 - $ 1595 10 99233 - $ 756 Total: $4305
Evaluation and Management Services Discharge Services • Two codes • 99238, 30 minutes or less • 99239, more than 30 minutes • Document time spent • It is appropriate to report hospital discharge on same day as nursing home admit
Critical Care 99291 , 99292
Critical Care • Do not code for less than 30 minutes • Use the table in CPT for correct coding • Does not have to be continuous time • Unit/floor time • Does not have to face to face time only • 99291 is only billed once per date of service • Patient status and care provided must both meet definition of critical
Medicare Consultations Effective January 1, 2010 Medicare will no longer cover consultation CPT codes. 99241 – 99245 Office/Outpatient 99251 – 99255 Inpatient
Evaluation and Management Services- Consultations For Medicare: New modifier to identify the actual admitting physician on record. AI (Two letters not alphanumeric)
HX EX M (T) 99251 PF PF S 20 99252 EPF EPF S 40 99253 D D L 55 99254 C C M 80 99255 C C H 110 HX EX MDM (T) 99221 D D S/L 30 99222C C M 50 99223 C C H 70 Medicare Consultations - Inpatient
99251 1.0 99252 1.5 99253 2.27 99254 3.29 992554.0 992211.92 992222.61 99223 3.86 Medicare Consultations – Inpatient2013 Work RVU
HX EX M (T) 99251 PF PF S 20 99252 EPF EPF S 40 These two levels do not map to an initial inpatient visit code. The subsequent hospital visit CPT codes must be used. HX EX M (T) 99231 PF PF S/L 15 99232EPF EPF M 25 Medicare Consultations - Inpatient
99251 1.0 99252 1.5 99231 .76 99232 1.39 Medicare Consultations – Inpatient2013 Work RVU
Correct Diagnosis Coding Basic Documentation Rules to Code by for Physician Practices When coding from the medical record or source document only code those items clearly stated; DO NOT code anything listed as • “possible”, • “probable”, • “maybe”, • “suspected”
Correct Diagnosis Coding Basic Documentation Rules to Code by for Physician Practices There are no “rule-out” codes
Correct Diagnosis Coding Basic Documentation Rules to Code by for Physician Practices Be as specific as possible; code acute conditions as “acute” and chronic conditions as “chronic” And be sure they are noted that way in the chart
Correct Diagnosis Coding Basic Documentation Rules to Code by for Physician Practices When a concise diagnosis cannot be made, code based on signs and symptoms • Signs and symptoms do not have to be separately listed if they are an integral part of the underlying diagnosis or condition already coded.