Download

1 / 23
240 likes | 578 Vues
Group B Streptococcus. Peter Nguyen MSIII. Etiology. Facultative encapsulated gram-positive diplococcus Produces a narrow zone of -hemolysis on blood agar Most strains are bacitracin resistant Positive CAMP test . Etiology. Serologic Strains

E N D
Group B Streptococcus Peter Nguyen MSIII
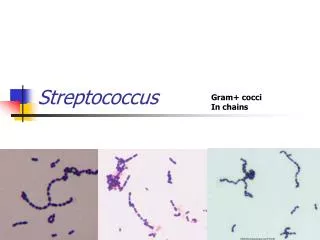
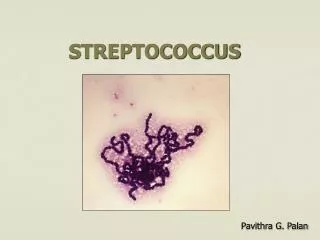
Etiology • Facultative encapsulated gram-positive diplococcus • Produces a narrow zone of -hemolysis on blood agar • Most strains are bacitracin resistant • Positive CAMP test
Etiology • Serologic Strains • Type Ia, Ib, Ia/c, II, III, IV, V, VI, VII, and VIII • Early onset disease can be due to any strain • Late onset disease is due to Type III in >90% of cases
Epidemiology • Colonizes ~20% of pregnant women • Usually asymptomatic but can have UTIs, chorioamnionitis, or endometritis • 40-70% of infants born to colonized mothers are colonized • Nearly 50% of sexually partners of colonized women are colonized themselves • 0.2-3.7/1000 live births • Rates are diminishing with prophylaxis • 0.5-2% of newborn infants born to colonized mothers
Risk Factors for Colonization • Heavily colonized mothers • Mothers younger than 20 • African Americans • Lower socioeconomic groups • PROM • Prolonged labor • Maternal Chorioamnionitis • Previous delivery with GBS disease
Occurs within the 1st week of life (usually <72 hours) Attack rate 1/birth weight Accounts for 20% Cases appearing up to 6 months of age Cases after 1 month of age occur primarily in premature and immunodeficient infants Early Onset v. Late Onset
Vertical transmission Ascending infection (duration of ROM incidence of infection) During passage through a colonized birth canal Maternal transmission Nonmaternal sites: Nursery Personnel Community Pathophysiology due to weakened host defense Early Onset v. Late Onset
Pneumonia with bacteremia Pulmonary HTN (COX) Meningitis Bacteremia without a focus (55%) Meningitis (35%) Osteomyelitis and arthritis Early Onset v. Late Onset
Differential Diagnosis • HMD • Amniotic fluid aspiration • Sepsis from other ascending infections • Metabolic and anatomic abnormalities that manifest as sepsis
Laboratory Findings • Isolation and identification from normally sterile sites • CSF • Gastric or tracheal aspirates • Skin or mucous membranes
Laboratory Findings • Latex particle agglutination • Less sensitive than culture • Useful in patient who has had prior antibiotic therapy, and is in sepsis without bacteremia
Laboratory Findings • Urine culture • Yields false positives due to colonization of healthy neonates in the perineum and rectum • Urine latex test • Do not perform on an asymptomatic patient
Treatment • DOC: penicillin G • Empirical ABX treatment with ampicillin and an aminoglycoside until GBS has been cultured • Also susceptible to: • Vancomycin • Semi-synthetic penicillins • Cefotaxime • Ceftriaxone • Impipnem
GBS Meningitis • Penicillin should be used in high doses (300mg/kg/day) for the treatment of GBS meningitis because of: • A high CSF inoculum • Relapse in patients treated with 200 mg/kg/day • The Relative safety of penicillin in neonates
GBS Meningitis • Obtain CSF culture within 48 hours of therapy induction • If growth is present, add an aminoglycoside to the treatment
Treatment Duration • Pneumonia: 10 days • Arthritis: 2-3 weeks • Osteomyelitis: 3-4 weeks • Endocarditis: 3-4 weeks
Recurrent Infection • Due to persistent mucosal colonization rather than a sequestered focus • Full course of penicillin and aminoglycoside followed by rifampin • Mother’s breast milk may be a source • Culture milk • Treat mother with rifampin
Supportive Care • Hypoxia and shock • DIC • Seizures • Increased ICP • SIADH
Complications • Mortality rate ranges from 5-15% • Highest in VLBW infants, those in septic shock or those who had a delay in therapy • Decreasing due to earlier dx and tx, increased intrapartum prophylaxis, and ECMO
Complications • Neurologic sequelae occur in 20-30% of meningitis cases • Mental retardation • Quadriplegia/hemiplegia • Seizures • Hypothalamic dysfunction • Cortical blindness • Hydrocephalus • Bilateral deafness
Laboratory Findings • Selective intrapartum chemoprophylaxis (SIC) • IV penicillin G or ampicillin at onset of labor or when PROM is anticipated (clindamycin for penicillin allergic patients) • Should be implemented in communities and hospitals where GBS perinatal disease is prevalent • Decreases the incidence of early-onset but not late-onset disease
Laboratory Findings • All infants whose mother received SIC should be observed for 48 hours for signs of infection • Neonatal infection: treatment continued for 5-7 days • Antibiotic resistance
Bibliography • Behrman, Richard E.; Kliegman, Robert; Jenson, Hal B. (1999) Nelson Textbook of Pediatrics, 16th ed Philadelphia: Saunders W.B. Co. • http://www.groupbstrep.org/