Download
1 / 50
500 likes | 504 Vues
This audit examines the availability and use of laboratory assays for toxins in the management of patients with potentially serious poisoning. It includes supportive investigations, availability of tests 24/7, and turnaround time for specific assays.

E N D
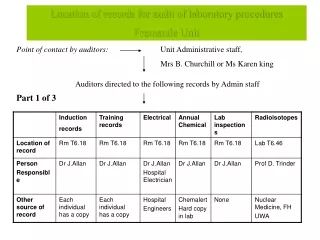
Surrey Pathology Services A joint venture between Ashford and St. Peter’s Hospitals NHS Foundation Trust,Frimley Health NHS Foundation Trust and Royal Surrey County Hospital NHS Foundation Trust National Audit of Laboratory Analyses for Poisoned Patients Dawn Grenshaw and Heather Stoddart 22nd June 2016
Background Poisoning is a common reason for presentation and admission to hospital. Most patients recover with little or no medical intervention, but a minority have more serious or life threatening poisoning. Laboratory assays for toxins are an important part of the management of patients with potentially serious poisoning. Availability and use of investigations varies between hospitals. Particular problem OOH.
National Audit - April 2016 • Audit questionnaire sent via ACB office to 471 ACB “non-trainee” members in UK and Republic of Ireland. • 82 responses • 26 teaching hospitals (31%) • 43 DGH (52%) • 5 Pathology Networks (7%) • 4 Tertiary Referral Centres (5%) • 4 Other (5%) • Specialised laboratory • Teaching Hospital and Tertiary Referral Centre • Laboratory services incorporate DGH and Teaching hospital through shared service
April 2016 Audit Location of Organisations: 59 in England (72%) 13 in Scotland (16%) 5 in Northern Ireland (6%) 3 in Wales (4%) 2 in Republic of Ireland (2%)
Supportive Investigations “Should be available on a 24-h basis to all hospitals where patients with acute poisoning are admitted” “…results should be available within a maximum of 2h of presentation.” FBC Na, K, urea, creatinine Glucose Ca, Alb, Mg INR ALT/AST Bilirubin Anion Gap (Cl, Bicarbonate) Plasma osmolality and osmolar gap. Arterial blood gases CK
Supportive Investigations Q2. Are the following tests available 24/7?
Supportive Investigations Q2. Are the following tests available 24/7? Blood gases available on acute wards, not in lab – 5 labs. Osmolality available out of hours on special request only/after discussion with on-call Consultant – 4 labs. Calculated osmolality available, measured osmolality available at another hospital within network. AST not routinely offered out of hours – 3 labs. AST sent away to another hospital. AST only available to gastroenterologists. Specialist laboratory only - these routine Biochemistry tests would be available within the Biochemistry Department at the same hospital.
Group 1 Assays “Assays that should be available on a 24-h basis in all acute hospitals” “Results should normally be available within a maximum of 2h of presentation” Carboxyhaemoglobin Digoxin Ethanol Iron Lithium Methaemoglobin Paracetamol Paraquat (qualitative urine test) Salicylate Theophylline Valproate
Group 1 Assays: Availability Only 38% of labs have paraquat available within lab/network; 23% not available at all.
Q3: Carboxyhaemoglobin All labs report COHb in %
Q3: Carboxyhaemoglobin Origins of reference ranges: Toxbase, Tietz, manufacturer, historical, unknown, Goldfranks Toxicology Emergencies. Q: Do you have a phoning limit for COHb? • >10%; >15%; >20%; >9%; >5% GP • All results phoned • Abnormal results phoned • All results requested urgently phoned
Q3: Carboxyhaemoglobin Annual Workload Range: 0 – 40,000 p.a. Median: 64 tests per annum
Q4: Digoxin – Units and Phoning Limit • Most labs report in mass units – 56 (89%) in g/L. • 4 labs nmol/L (6%) • 3 labs ng/mL (5%) • 62 labs (97%) have a telephone limit for digoxin.
Q4: Digoxin Reference Ranges • Source: • Pathology Harmony (14 labs) • Manufacturer (4 labs) • Unknown (3 labs) • Adapted from Syva 1981 • Hallworth & Watson – Therapeutic Drug Monitoring • ESC Guidelines 2008 • Local
Q4: Digoxin Annual Workload Range: 0 – 5000 p.a. Mean: 1192 p.a.
Q4: Digoxin – Digibind policy? Do you have a policy, procedure or recommendation for digoxin measurement in patients receiving digoxin-specific antibodies (Digibind)? Yes – 34 labs (54%) No – 29 (47%) Policy/Procedure/Recommendation Comment on report stating digoxin unreliable: 5 labs Known to interfere with the assay. We recommend measuring digoxin prior to use: 5 labs Question asked on Order Comms system about Digibind and comments made accordingly – 2 labs. Would not recommend measuring digoxin for a stated period of time (48h, 7 days, 10-14 days, 3 weeks) – 4 labs Trust policy on Digifab states do not measure digoxin post-treatment – 1 lab Lab staff aware of interference and information provided in lab handbook – 1 lab
Q5: Ethanol - Units “The use of different units for reporting plasma ethanol concentrations is confusing and potentially dangerous. The recommended units for reporting ethanol concentration are mg/L.” • g/L • mg/dl but soon changing to mg/L 31%
Q5: Ethanol – Workload per year Range: 0 – 12,629 p.a. Mean: 1490 p.a. Median: 450 p.a.
Q6: Iron • Haemolysed samples: • 40 labs (69%) reject all haemolysed samples • 18 labs (31%) accept haemolysed samples • Desferrioxamine: • All labs (58 that responded) use colorimetric assays. • 45 labs (78%) have no policy/recommendation for iron measurement in patients receiving desferrioxamine. • 13 labs (22%) have a recommendation: • Would advise assay not suitable – 5 labs • Would advise that iron results may give artificially low results – 3 labs • Advise wait 2h after cessation of infusion before measuring iron – 1 lab • ICP-MS analysis of iron available or urine iron – 1 lab • No formal policy but the Duty Biochemist would contact the ward for iron overload cases – 1 lab • Therapy continues until serum iron falls below TIBC or urine loses its pink colour – 1 lab • Suggest use ferritin – 1 lab
Q6: Iron – Annual Workload Range: 1 – 81,745 p.a. Mean: 16,828 p.a. Median: 6653 p.a.
Q7: Lithium Telephoning Limit for Lithium: 60 labs (97%) have a phoning limit 2 labs (3%) do not.
Q7: Lithium – Annual Workload Range: 0 - 5874 p.a. Mean: 2275 p.a.
Q8: Methaemoglobin Annual Workload 22 labs – done on all blood gases (POCT) Range: 0 – 48,000 p.a. Median: 17 p.a.
Q9:Paracetamol Annual Workload Range: 1 - 6000 p.a. Mean: 2497 p.a.
Q10: Paraquat: Turnaround Time 38% of labs offer same day qualitative urine paraquat; 27% in <4 hours
Q10: Paraquat Annual Workload • 0 in 10 years • 0 in 3 years • 1 in the last 5 years • I don't remember the last request • It is now several years since a request for this investigation • Never been requested (not since 90's) • No data but very few, not more than 2-3 per year. • Tiny
Q10: Paraquat Training and Competency 21 labs commented: Training not provided - 3 labs Some sort of training/competency exercise in place – 17 labs Restricted to a small number of staff who are competent and called out when required – 6 labs All state registered staff trained and signed off as competent – 6 labs Annual reassessment of competency (6 monthly in one case) : 3 labs Spiked urine sample/positive control: 4 labs With difficulty. Staff perform an assay using stored weedol which until now has always given a positive result and a negative test. Not rigorous. Assay is likely to be made obsolete in light of ISO 15189
Q10: Paraquat Training and Competency Re-establishment of the method planned as part of regional requirement. Update training provided every 6 months along with ad hoc training every time a sample comes in for paraquat/diquat analysis. 6 staff are trained to provide 24/7 cover for Northern Ireland. All are experienced BMS/CS staff Band 7 and above. Competency forms are completed by staff at each update training session. We have had several positive cases over the last few years from both accidental and deliberate paraquat/diquat ingestion so staff do get to see positive cases.
Q11: Salicylate Annual Workload Range: 1 - 5197 p.a. Mean: 1911 p.a.
Q12: Theophylline Units: mg/L - 61 labs (97%) mol/L – 2 labs (3%) Phoning Limit: Yes – 57 labs (89%) No – 7 labs (11%) Phoning Limit used: 25 mg/L – 39 labs (68%) 20 mg/L – 8 labs (14%) 30 mg/L – 2 labs (4%) 45 mg/L – 2 labs (4%) Others (1 lab each): 22 mg/L 23 mg/L 150umol/L >20.0 mg/L (>15.0 mg/L for neonates <28 days old) >25 (adult) >10 (neonate) >25mg/L adults; >20mg/L <17y/o
Q12: Theophylline Annual Workload Range: 1 - 3300 p.a. Mean: 636 p.a.
Q13: Valproate Units: mg/L – 57 labs (93%) mol/L – 3 labs (5%) g/mL – 1 lab (2%) Telephoning Limit? No – 46 labs (74%) Yes – 16 labs (26%) Phoning Limit Used: 100 mg/L – 6 labs 150 mg/L – 5 labs 200 mg/L – 1 lab 20 mg/L – 1 lab 280 mg/L – 1 lab 120 mg/L – 1 lab 850 mg/L – 1 lab
Q13: Valproate Annual Workload Range: 0 – 2000 p.a. Median: 345 p.a.
Group 2 Assays “Arrangements should be in place so that these assays can be accessed urgently when necessary.” “It is the responsibility of each individual hospital to ensure that appropriate arrangements are in place and that staff can follow these arrangements when the need arises, including outside normal working hours.” Arsenic Carbamazepine Cholinesterase (plasma and erythrocyte) Cyanide Ethylene Glycol Lead Mercury Methanol Methotrexate Paraquat (quantitative plasma) Phenobarbital Phenytoin Thallium Thyroxine Toxicology Screen
Group 2 Assays: Turnaround Time Urgent results in <2h Result should be available in <4h Urgent plasma result <3h, inc journey time; red cell <6h Urgent result should be available within 2h Result within 2-4h
Group 2 Assays Q: If this test is referred, do you have a formal agreement with the referral laboratory to provide analysis urgently in cases of suspected poisoning?
Group 2 Assays: Annual Workload 733 Mean Annual Workload 371 110 112 17 6 3 13 2 9 6 0.1
Group 2 Assays: Toxicology Workload Range: 0 – 21,000 p.a. Mean: 1611 p.a. Median: 168 p.a.
Q14: Carbamazepine Units: mg/L – 60 labs (98%) mmol/L – 1 lab (2%)
Units: mg/L – 58 labs (95%) mol/L – 3 labs (5%) Source of reference range: Pathology Harmony – 15 labs Historical/unknown – 4 labs Manufacturer – 3 labs Patsalos et al 2008.Epilepsia, 49(7):1239-1276 (10 – 20 mg/L, 1 lab) Alan Richens (best control 10 – 20 mg/L, 1 lab) Therapeutic Drug Monitoring Publishers ACB Venture Publications 2008 (10 – 20 mg/L, 1 lab) Q16: Phenytoin
Q16: Phenytoin Phoning Limit? Yes – 53 labs (90%) No – 6 labs (10%)
Summary of Findings • Supportive Investigations • Most supportive investigation are available 24/7 in most laboratories. • A few labs do not offer AST, or it is not offered routinely. • A few labs do not offer osmolality 24/7 or it is only available after approval by a consultant.
Summary of Findings • Group 1 Assays • Most analytes are available locally at most laboratories, although quoted TATs varied. • There is variation in reference ranges for carboxyhaemoglobin and digoxin. • Only half of the laboratories surveyed had a policy for measurement of digoxin in patients who have been given Digibind. • Most laboratories did not have a policy for iron measurement in patients who have been given desferrioxamine. • Ethanol is widely reported in mg/dL, rather than the recommended mg/L. • Urine paraquat testing is an issue.
Summary of Findings • Group 2 Assays • The majority of laboratories offered all the required analytes, either in house or by referral, although thallium, cyanide and quantitative plasma paraquat were less likely to be available. • With the exception of carbamazepine, phenytoin and thyroxine, very few analytes were available urgently in the majority of labs. • Few labs have formal arrangements for urgent analysis with referral labs, although about 1/3 of labs had some kind of arrangement in place for ethylene glycol and methanol.
Thank you: • Heather Stoddart • TAG committee • Mike Lester, ACB Office • All the laboratories who participated in this audit