Download
1 / 11

E N D
Diabetes Insipidus Ovidiu Galescu MD
Definition • Diabetes insipidus (DI) is an uncommon condition that occurs when the kidneys are unable to conserve water as they perform their function of filtering blood. The amount of water conserved is controlled by antidiuretic hormone, also called vasopressin.
Central and nephrogenic • ADH is a hormone produced in a region of the brain called the hypothalamus. It is then stored and released from the pituitary gland, a small gland at the base of the brain. • DI caused by a lack of ADH is called central diabetes insipidus. When DI is caused by a failure of the kidneys to respond to ADH, the condition is called nephrogenic diabetes insipidus.
Symptoms of DI • Polyuria, • Nocturia, • Thirst Thirst is essential so that the excess urinary water losses can be replaced. Patients without an intact thirst mechanism can develop severe hypernatremia.
Diagnosis • A high-normal plasma sodium concentration (greater than 142 meq/L • Urine osmolality less than the plasma osmolality • Water restriction test
The normal physiologic response to the water restriction test • Raising the plasma osmolality leads to a progressive elevation in ADH release and an increase in urine osmolality in normal individuals. • Plasma osmolality at 295 to 300 mosmol/kg (normal 275 to 290 mosmol/kg) or the plasma sodium > 145 meq/L the effect of endogenous ADH on the kidney is maximal. • DDAVP has no effect unless endogenous ADH release is impaired (ie, unless the patient has central DI).
Test end: • Urine specific gravity ≥1.020 • Urine osmolality is ≥600 mosmol/kg • Plasma osmolality > 295/300 mosmol/kg or Na i> 145 meq/L • The patient has lost 5 percent of body weight or exhibits signs of volume depletion • If > 6 hours in infants less than six months of age, 8 hours in children from six months to two years of age, or 12 hours in children older than two years of age
Interpretation – central DI • DDAVP leads to a rise in urine osmolality (and an equivalent fall in urine output) of more than 100 % in complete central DI and 15-50% in partial central DI
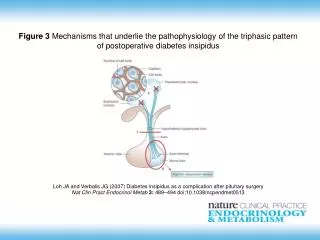
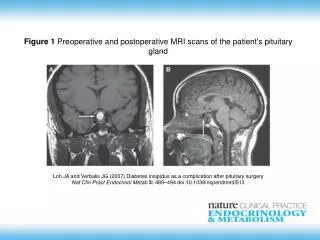
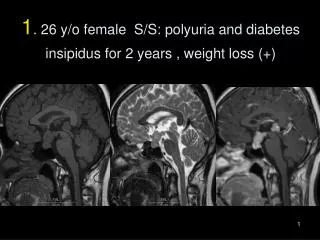
Central DI • Damage to the hypothalamus or pituitary gland • Head injury • Infection • Loss of blood supply to the posterior pituitary gland • Surgery • Tumor There is also a form of central diabetes insipidus that runs in families.
Central diabetes insipidus • Characterized by decreased release of ADH • Insult at sites involved in ADH secretion • the hypothalamic osmoreceptors; • the supraoptic or paraventricular nuclei; or • the superior portion of the supraopticohypophysealtract
Treatment - Risk of hyponatremia • Although thirst will be suppressed by effective therapy, much of the fluid intake during the day is not driven by thirst • Previously untreated patients may have become accustomed to drinking large amounts of fluids and may continue to do so for a short period after the initiation of effective therapy. • The initial aim of therapy is to reduce nocturia, thereby providing adequate sleep, most often by the administration at bedtime