Download
1 / 45
480 likes | 597 Vues
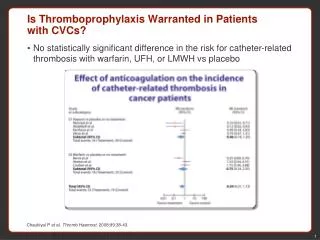
Thomas Li Consultant respiratory physician Union Hospital. Thromboprophylaxis in ICU. Receive no sponsorship from any drug company or medical device company Declare no conflict of interest with any drug company or medical device company. Guidelines of VTE prophylaxis

E N D
Thomas Li Consultant respiratory physician Union Hospital Thromboprophylaxis in ICU
Receive no sponsorship from any drug company or medical device company Declare no conflict of interest with any drug company or medical device company
Guidelines of VTE prophylaxis • Development of local guideline • Mechanical methods of VTE prophylaxis • Other strategies for early detection of VTE • Routine USG screening • Low threshold CTPA • Restriction of sedation • Early rehabilitation
International guidelines • American College of Chest Physicians • Surviving Sepsis Campaign • Institute of Healthcare Improvement • National Institute of Health and Care Excellence
Who are at risk ? • Medical patients • Mobility significantly reduced ≥ 3 days • Reduced mobility + any VTE risk • Surgical patients • Anaesthetic time > 90 minutes • Anaesthetic time > 60 minutes + operation involves pelvis or lower limb • Acute surgical admission with inflammatory or intra-abdominal • Expected reduced mobility • Any VTE risk factors NICE guideline
Increased risk of VTE • Active cancer or cancer treatment • Age > 60 years • Intensive care admission • Dehydration • Known thrombophilia • BMI > 30 • 1 or more significant medical comorbidity • Personal or family history of VTE • Use of HRT or contraceptive • Varicose veins with phlebitis NICE guideline
Increased risk of bleeding • Active bleeding • Acquired bleeding disorders eg liver failure • Concurrent use of anticoagulant • LP, epidural or spinal anaesthesia in coming 12 hours • LP, epidural or spinal anaesthesia within past 4 hours • Acute stroke • Platelet < 75 • BP > 230/120 • Untreated inherited bleeding disorders
Position statement on prevention of VTE in ICU in HK • Local epidemiological studies without pharmacological prophylaxis • Mixed ICU patients: 11% with femoral vein cannulation had iliofemoral DVT (Joynt et al. CHEST 2000) • Medical ICU patients: 8% above knee DVT, 11% below knee (Joynt et al. HKMJ 2009)
Other Asian countries • 10.5% (20/190) surgical ICU patients without thromboprophylaxis in Thailand had DVT • 4.7% (9/190) were proximal DVT • 3.7% (7/190) had PE confirmed by CT (Asian J Surg 2009;32:85) • In a neurorehab ward in Singapore • 98% not on heparin • 77% Chinese, 14% Malay, 7% Indian • Proximal DVT 2.6%(11/419), distal 2.4%(10/419) (Arch Phys Med Rehabil 2008)
Position statement on prevention of VTE in ICU in HK • Graduated compression stockings (GCS) and intermittent pneumatic compression (IPC) devices are commonly used • Most except a few ICUs use pharmacological DVT prophylaxis
Position statement on prevention of VTE in ICU in HK • No RCT on prevention of VTE in Chinese critically ill patients could be identified • 5 RCT on prevention of VTE in Chinese patients could be identified
Thromboembolic prophylaxis for TK arthroplasty in Asian patients > 90% were ethnic Chinese Journal of Orthopaedic surgery 2009
Thromboembolic prophylaxis for TK arthroplasty in Asian patients
LMWH as DVT prophylaxis for Asian colorectal surgical patients • Enoxaparin 20 mg Q12H preop • Enoxaparin 40 mg daily for at least 4 days post-op • 5/169 in control group had DVT, 3 out of the 5 DVTs also had acute pulmonary embolism • 0/134 on enoxaparin had DVT/ PE (P=0.045) • 3/169 in control had bleeding related complications • 9/169 had bleeding complications (1 subdural haematoma and 2 intra-abdominal bleed exploration) (P=0.037) • Authors supported use of LMWH Dis Colon Rectum 1999
DVT in HK Chinese with hip fractures: Incidence and effects of LMWH 37% (29/ 78) developed DVT No difference in incidence between 2 groups LMWH may reduce proximal DVT Arch Orthop Trauma Surg 1999
Position statement on prevention of VTE in ICU in HK • Best available evidence do not address the benefits and risks of Chinese critically ill patient regarding pharmacological prophylaxis • RCT in Chinese critically ill patients are needed
What else can we use to prevent/ manage DVT or VTE ? • Mechanical devices • Routine screening • Low threshold for CT • Early mobilization
How effective in mechanical devices ? • Systemic review • MEDLINE, EMBASE, Biosis, Derwent • Mostly surgical patients • Mechanical devices (GCS or IPC or foot pump) • reduce risk of DVT by 2/3 as monotherapy • reduce risk of DVT by ½ when combined with pharmacological prophylaxis • reduce risk of proximal DVT by ½ • Reduce risk of PE by 2/5 Health Technology Assessment 2005
ACCP 2008 guideline • Appropriate size • Proper fitting • Compliance • Storage • Disinfection
Is graduated compression stocking (GCS) harmless ? • CLOTS 1 study • Multi-centre, international, UK, Australia and Italy • 2518 patients admitted to hospital within 1 week of onset of acute stroke • > 80% were ischaemic stroke • Randomized thigh length GCS or control • USG at day7-10 and day 28-30 CLOTS trial collaboration Lancet 2009
Is graduated compression stocking (GCS) harmless ? GCS Control Proximal DVT 10% 10.5% Skin ulcers Blisters 5% 1% Necrosis
CLOTS 2 trial: Thigh-length vs below knee stockings for DVT prophylaxis after stroke • Multi-centre, international randomized • 3114 patients hospitalized within 1 week of acute stroke (>80% were ischaemic) • Thigh length DVT or below knee DVT • Prematurely stopped enrollment because of results of CLOTS 1 trial Ann Intern Med 2010
CLOTS 2 trial: Thigh-length vs below knee stockings for DVT prophylaxis after stroke Thigh length Below-knee Proximal DVT 6.3% 8.8% P=0.008 Death 10.9% 10.3% Any skin Problem 9% 6.9% P=0.03 Skin Breakdown 3.9% 2.9%
Why ? • Risk of DVT • No stocking = Thigh length stocking < below knee stocking • ? Increased risk of DVT with below knee DVT • If we believe the results, avoid the use of GCS for DVT prevention in patients after stroke
Why screen for DVT ? • It is present among our patients, but may be of lower prevalence than other ethnic groups • Controversy in use of pharmacological prophylaxis • Some patients have obvious contraindication to heparin or LMWH and may need IVC filter • It is clinically silent
DVT is clinically silent in ICU 239 patients surgical-medical ICU patients Twice weekly USG Structural clinical examination DVT risk score calculated Journal of Critical Care 2005
DVT is clinically silent in ICU • DVT risk scores used in symptomatic outpatients were not applicable in ICU • Universal prophylaxis or routine screening
Potential risk factors in critically ill Chinese medical ICU patients Only 4/15 of Confirmed DVT had signs 11/15 had no signs Joynt et al HKMJ 2009
Routine USG screening for DVT • Very few ICUs have access to portable ultrasound for diagnosis of DVT • Impractical to transport critically ill patients to radiological department regularly & frequently for ultrasound examination • Can intensivists do USG for diagnosis ?
A common scenario when I am on call in ICU • One night at 2 am, an ICU nurse call you patients in bed 1, 4, 5 and 7 have “desaturations” • What will be your reply ?
Your reply • Ask the nurse to continue observation & sleep • Examine each patients and reassure the nurse • Examine each patients + ECG • Examine each patients + ECG + portable CXR • Examine each patients + ECG + portable CXR + wake up the on-call radiologist for urgent CT pulmonary angiogram
Continuous SpO2 and diagnosis of pulmonary embolism in critically ill trauma patients • Continuous SpO2 monitoring and static lung compliance • >10% drop in SpO2 and no change in compliance • 48 out of 972 critically ill trauma patients in 18 months • 44% of these patients had PE demonstrated using pulmonary angiogram J Trauma 2001
Virchow’s triad • Hypercoagulability • Haemodynamic changes (Stasis or turbulence) • Endothelial damages or dysfunction
Daily interruption of sedation Kress et al. NEJM 2000
No sedation for critically ill on mechanical ventilation: RCT Lancet 2010
Early mobilization in ICU Lancet 2009
Recommendations • Multidisciplinary approach to prevent VTE • Early mobilization and rehabilitation • Reduction in use of sedatives and muscle relaxants • Compression devices for patients with high bleeding risks • Avoid femoral vein cannulation • Frequent regular USG screening for DVT
Recommendations • Remove central venous catheters as soon as possible • Low threshold for CT pulmonary angiogram for unexplained hypoxaemia • Consider pharmacological prophylaxis after balancing the risks and benefits
What the colleges and society can do ? • Encourage collaboration between different ICU for multicenter studies on local Chinese patients • Liaise with college of radiology to organize recognized training in ultrasound diagnosis of DVT for intensivists