Download
1 / 31
340 likes | 404 Vues
Congenital Dyserythropoietic Anemias. FEATURES COMMON TO ALL CDAs. The congenital dyserythropoietic anemias (CDAs) are a group of relatively rare inherited anemias that share common features:. FEATURES COMMON TO ALL CDAs. Anemia: mild to moderate ( Hb = 8-11 g/dl).

E N D
FEATURES COMMON TO ALL CDAs • The congenital dyserythropoietic anemias (CDAs) are a group of relatively rare inherited anemias that share common features:
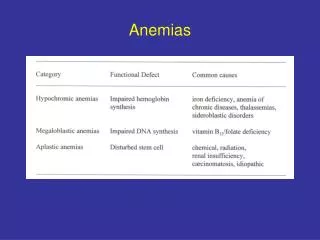
FEATURES COMMON TO ALL CDAs • Anemia: • mild to moderate (Hb = 8-11 g/dl). • Normocytic or macrocyticindicies are typical.
FEATURES COMMON TO ALL CDAs • Ineffective erythropoiesis: • The red cell half life is decreased to a variable extent in these disorders. • Granulopoiesis and thrombopoiesis are generally unremarkable
FEATURES COMMON TO ALL CDAs • Iron overload: • Increased plasma iron turnover. • Shortened half-life of plasma iron clearance.
FEATURES COMMON TO ALL CDAs • Multineucliarerythroid cells in B.M.
FEATURES COMMON TO ALL CDAs • Abnormalities of mature erythrocytes, including anisocytosis, poikilocytosis, and anisochromasia can be pronounced. • Reticulocytes are usually normal or slightly increased in number
FEATURES COMMON TO ALL CDAs • Three major types of CDA and a number of variants have been described. • The diagnosis and categorization of these disorders are facilitated by microscopic examination of the blood and bone marrow and by serologic testing.
SPECIFIC FEATURES OF CDA I • AR, Codanin-1 • Manifests in early infancy, childhood & sometimes adolesance . • mild to moderate macrocytic anemia Hct 30%
SPECIFIC FEATURES OF CDA I • Mild hyperbillirubinemia. • Splenomegaly.
SPECIFIC FEATURES OF CDA I • Hypercellularerythroid marrow with megaloblastoid features: 1- v. Large cells containing an irregular nuclear mass with 2 segments. 2- Double nucleated cells. 3- Pairs of erythroblasts connected by a chromatin bridge.
SPECIFIC FEATURES OF CDA I • E.M: A- multiple nuclear membrane pores. B- uneven condensation of chromatin, leading to a “spongy” nuclear configuration (characteristic)
SPECIFIC FEATURES OF CDA II • HEMPAS (hereditary erythroblastic multinuclearity with positive acidified serum lysis test). • Most common type.
SPECIFIC FEATURES OF CDA II • AR, Defect in the surface membrane gluco-conjugated proteins (chrom. 20) • (N-acetyl-glucosaminyl-transferase II) • (alpha-mannosidase II) • Mean age of presentation 5y.
SPECIFIC FEATURES OF CDA II • Mild to severe anaemia (variable) • Splenomegaly & Jaundice are more prominent. • Iron overload is the most serious complication. • Hepatomegaly.
SPECIFIC FEATURES OF CDA II • +ve acidified serum test • Not to its own serum (+ve to ABO comp. Serum) • Succ. Lysis test –ve. • Anti-i and anti-I agglutinability +ve.
SPECIFIC FEATURES OF CDA III • AD, chrom 15 • Usually asymptomatic. • Absent or minimal anemia. • N or minimal splenomegaly.
SPECIFIC FEATURES OF CDA III • Giant erythroblasts with upto 12 nuclei • E.M. Clefts in nuclei, autolytic areas in cytoplasm
Management • Anemia is often mild and requires no intervention. • Blood transfusion should be avoided unless necessary. • Splenectomy may be of benefit (CDA II).
Management • Patients should be routinely monitored for evidence of iron overload • Iron chelation therapy should be considered in the management of these patients after documentation of tissue iron overload.
Management • Identify family members. • Genetic counseling.