Download
1 / 50
500 likes | 795 Vues
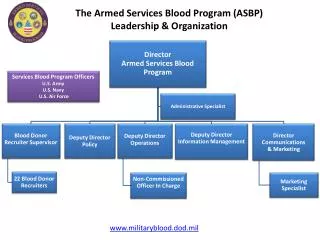
Armed Services Blood Program. www.militaryblood.dod.mil. UNCLASSIFIED. Society of Armed Forces Medical Laboratory Scientists. Armed Services Blood Program - Transformation -. CDR Michael C. Libby Director, Armed Services Blood Program Office. 12 Feb 08. Armed Services Blood Program.

E N D
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Society of Armed Forces Medical Laboratory Scientists Armed Services Blood Program- Transformation - CDR Michael C. Libby Director, Armed Services Blood Program Office 12 Feb 08
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Purpose To provide thoughts on what might be ahead for the ASBP in order to be far more efficient in using available resources. To get people to start thinking about the big picture of the certain business change. To raise a broad suggestion about where the Armed Services Blood Program is going over the long term and what are the underlying forces creating transformation. To succeed we need to operate beyond the edge of knowledge where time honored rules of thumb might not apply in the organization.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Briefing Outline To put the transformation in proper perspective, the ASBP will be described in a history capsule from 2001 to 2008. • Where we have been. • Where we are now • Where are we going… We are on the verge of a historic shift… a National Blood Program? Accelerated technological and business changes are in the foreseeable future and will bring similar gov’t agencies together.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Senior Military Medical Advisory Committee Blood ProgramBusiness Case Analyses Toward a Future State March 2003 ( A STEP BACK IN TIME!)
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED - ASBPO Convened SME Panel 24-27 April 2001 • Lt Col Ruth Sylvester, USAF, Chair • Lt Col Fabrizio Saraceni, USAF; CDR Brenda Bartley, USN; LCDR Michael Libby, USN; Maj Donna Whittaker, USA; Maj Ken Pell, USA - ASBPO Convened SME Panel 21-22 June 2001 • Lt Col Ruth Sylvester, USAF, Chair • Lt Col Fabrizio Saraceni, USAF; CDR Brenda Bartley, USN; LCDR Michael Libby, USN; Lt Col (P) Gary Norris, USA; Ms Kathleen Elder, USA
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED 2001: Why A Strategic Plan Based on a BCA? • ASD(HA) tasked ASBPO to develop plan to deal with vCJD deferral looming over horizon (Mar 01) • * GOAL – maintaincontingency/peacetime needs. • Tasking two-fold • Short term (3-6 mo) plan of action (POA) to deal w/ vCJD deferral criteria (over 25% expected) • Long term strategic plan for ASBP to meet peacetime/wartime blood needs in efficient, cost effective and regulatory compliant manner • Support w/ POA, milestones, timeline & BCA
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED 2001: Short Term Recommendations • Make up estimated 25% vCJD donor deferral • Obtain donor recruitment resources • Eliminate non-productive screening of ineligible donors • Minimum of 16 recruiters needed • Obtain additional phlebotomy resources • Place at select CONUS BDCs at training sites • Minimum 10 phlebotomists needed
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED 2001: Long Term Recommendations • Hire contractor to conduct BCA to validate panel findings and to: • Determine optimum number of BDCs & testing centers • Determine optimum locations for assets • Develop long term strategic plan based upon outcome of BCA
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED March 2003Blood Program Mission (1) (1) ASWBPL West shipments OCONUS ASWBPL East shipments OCONUS • Mission is to collect blood in CONUS to support the warfighter overseas • One output of this program is a cost effective peacetime blood supply • Blood products collected were not linked to an established mission to support peacetime needs of the Region or MHS
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED March 2003Define Peacetime Mission of ASBP • Establish goal of DoD blood supply self sufficiency in peacetime needs • Staff and resource to meet peacetime blood needs • Transfusion, ASWBPL quotas, and normal shelf inventory and expiration • Total program goal: 85,000 usable units/year (150,000/year in 2005-08) • Requires 106,000 total donors/year (180,000/year) • Build in flexibility for surge expansion Existing cost data show that a peacetime blood mission based on these criteria would be cost effective
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Cost Comparison Cost per unit of blood acquired DoD Readiness $ 68 DoD Peacetime Acquisition $ 143 (Average Total Cost $ 211 Range) $ 175 – 300) Civilian Acquisition ~ $ 210 (Range $ 175 – 250) DoD acquisition cost for blood in peacetime is considerablylower than civilian acquisition cost but there is wide variation in both. Cost per unit of blood transfused DoD Readiness $ 68 Civilian Transfusion $ 500 DoD Transfusion $ 635 DoD transfusion costs appear higher than civiliantransfusion costs but the source of variation is not clear.
Armed Services Blood Program 12,404 to Civilian 10,258 from Civilian Civilian Blood Programs 1,254 to Army 3,915 to Civilian 1,555 to Navy 6,846 from Civilian NAVY 19,118 donations ARMY 12,332 4,615 to Civilian 51,218 donations transfusions 7,956 from Civilian 30,176 transfusions 4062 3583 ASWBPLs CY00 data. Frozen blood, manufacture of blood products omitted for clarity 3661 656 to AF 632 to Navy 529 to Army 3,400 to VA 2,933 to AF AIR FORCE 48 from VA 18,933 donations 12,780 transfusions 1,107 to VA 33 from VA 3,754 to VA 78 from VA VA Hospitals www.militaryblood.dod.mil UNCLASSIFIED March 2003: ASBP Annual External / Internal Exchange More units of RBCs are transferred OUTSIDE the ASBP (to / from civilian agencies, VA) than are transferred between Services inside the Program
Armed Services Blood Program March 2003: Command, Control, and Funding Line (Installation Commander) Service-specific Medical Service Surgeon General Health Affairs MTF CO Armed Services Blood Program Office Service Blood Program Officer Chief OIC Medical Treatment Facility FDA Licensed Program Ancillary Services JCS J4 (HSSD) Blood Donation Center Blood Transfusion Center Typical reporting structure Some BDCs are stand-alone or use other staffing arrangements COCOMS • Blood Program has responsibility but no authority for resources • Blood donor centers compete with health care delivery for funds and staffing
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Mar 03: Short-Term Improvements to Increase Efficiency • Increase recruiters, phlebotomists, & MLTs, to optimize collection/production of blood products • Move to a data-driven management process • Develop a needs and inventory visibility system • Develop targeted quarterly communications for overall program & donor communities • Optimize blood credit system across Services
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Mar 03: Improvements Discussed Long-Term • Optimize BDC site location • Redefine peacetime mission requirements for BDCs • 100% of DoD needs (125K annually) • Contingency (2100 units/day) • Create mechanisms to balance blood inter-regionally and inter-Service in peacetime • Separate blood manufacturing program from health care delivery to align authority with accountability • Separate budget for BDCs from core medical budget • Separate staff for BDCs from MTF laboratory • Successful models – ASBBCs, Ft Hood & Ft Knox • Implement incentive based funding
Armed Services Blood Program SG SG SBPO SBPO SG SG SG MTF MTF BDC BDC SBPO SBPO SBPO Standardized Data BDCs BDCs BDCs BDCs are Multi-Service Staffed as Appropriate Separate budget for BDCs www.militaryblood.dod.mil UNCLASSIFIED Recommended Program Rationalize and Consolidate BDC Site Locations Administrative management of inventory BDC staff report to SBPOs Redefine Peacetime Mission Maintain Service FDA Licenses Standardize data reporting and leverage existing systems AIR FORCE ARMY NAVY
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED - GWOT/OIF OEF Years - National Security and Emergency Preparedness The 2003 to 2008 Gap in Executing a Business Plan
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED The 2003 to 2008 Gap in Executing a Business Plan • ASBP Strategic Planning Workshops were held in 2003 to 2004. • ASBP Workshops On Developing Capabilities and Strategic Planning held each year from 2005 to present. In 2008, the Workshop have representatives from NATO and an executive session with J4 and ASD(HA)FHP&R.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Blood Products for OEF/OIF as of 27 May 03
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED OIF Transfused Blood Products
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Vision Tenet: War Focused Operation Iraqi Freedom and Operation Enduring Freedom Global War on Terrorism/Operations • Improve the mortality and morbidity of battlefield casualties by developing products that can be used by medics and physicians far-forward of a field hospital. • American forces in the Iraq and Afghanistan conflict are experiencing the highest casualty survival rate in U.S. history. • Mitigate the risk of emergent battlefield blood product transfusion to trauma casualties that include post-deployment medical care. Tomorrow’s Science for Today’s Warfighters
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Challenges • Changing doctrine in tracking post-transfusion patients and creating tracking systems • The recipients of our transfusion services: • US Military • Civilians from multiple nations • Coalition military partners • NATO military partners • US Gov’t Civilians • US Citizens (contractors, others) • US Citizens receiving blood products from non-US hospitals
Armed Services Blood Program Blood Product Transfusions by Nationality 11% 31% 54% 4% 69% of blood products are transfused to non-U.S. forces As of 31 August 2007
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Challenges The physician practice of collecting and transfusing “fresh” whole blood and apheresis platelets supports aggressive hemostatic resuscitation techniques performed in parallel with aggressive surgical control of bleeding. • Develop blood products to support • damage control resuscitation in lieu • of fresh whole blood. • Develop rapid screening field tests for transfusion transmitted diseases, ABO Rh, and patient-donor compatibility.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Challenges – Transfusion Medicine Transfusion practices in CENTCOM arise: • RBC age effect on massive transfusion in trauma. • Use of deglycerolized RBC in massively transfused patients. • Component therapy vs whole blood transfusions. • RBC to FFP ratios (use of AB plasma vs A plasma). Issues in the US: • Convalescent plasma • TRALI • DBL RBC collections • ETC, ETC
Armed Services Blood Program 2005: ASBPO partners with US Government A vital component of US medical support DOD: Provides Patient Movement Definitive Care DHS: Provides Funding VA: Provides Definitive Care HHS: Provides Response Teams
Armed Services Blood Program Disaster Occurs Local first responders react City requests aid from state Governor requests Presidential Disaster Declaration through DHS DHS implements National Response Plan President declares major disaster or emergency NORTHCOM Responds (when directed) JTF et al Secretary of Defense authorizes DoD support DHS requests DoD support Defense Support to Civilian Assistance Process ASBP engaged in scenario planning/ Execution of NRP.
Armed Services Blood Program Department of Defense Dept, Health and Human Services National Response Plan QDR MRR Strategy for Homeland Defense and Civil Support National Infrastructure Protection Plan JCS J4 HSSD FDA ASBPO CDC NIH ASD(HA) FHP&RP2 Homeland Security Homeland Defense ASPR ASH NORTHCOM TRANSFORM THE FORCE/UNITY OF EFFORT
Armed Services Blood Program Quadrennial Defense Review Roadmap for Medical Transformation 15 June 2006
Armed Services Blood Program QDR 3: Homeland Defense and Medical Civil-Military Operations Objective: Align MHS capabilities to meet the requirements of DoD Homeland Defense, civil support, and medical civil-military operations. Task 2: In FY 2007, use Joint Capabilities Integration and Development System (JCIDS) to conduct a capabilities-based analysis to determine the MHS “DOTMLPF” requirements. * ASBPO is a member of the JS War Eagles, a JCIDS advisory group to Force Health Protection Board / Functional Capabilities Board (Ms Embrey). Provide the Joint Force with the capabilities needed to perform across the range of military operations and challenges. Achieving Unity of Effort: All gov’t agencies to integrate their efforts into a unified strategy.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED MHS: Homeland Defense and Civil Support Ensure medical capability for homeland defense and civil support missions. Driven by: • Strategy for Homeland Defense and Civil Support • Hurricane Katrina Lessons Learned • DoD Quadrennial Defense Review (QDR) MHS Initiative #3 Fulfill DOD responsibilities under National Response Plan (NRP) • DOD is a supporting agency to all Emergency Support Functions (ESFs), including ESF #8 (Public Health and Medical Services) Engage the interagency in transforming our national capacity to manage the public health and medical aspects of catastrophic domestic events • Position the Emergency Medical System to surge into a “Disaster Medical System” when needed. *2008, CIVILIAN BLOOD COLLECTION AGENCIES ARE NOT MENTIONED IN ESF #8. INCREASES RELIANCE ON DOD BLOOD PROGRAM AS A GOV’T ASSET.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED MHS Preparedness – Way Ahead Need a process to create a National system to understand population(s) at risk and determine the requirement(s) for medical countermeasures. • Necessarily includes Federal, state, and local governments, as well as national pharmaceutical manufacturing base and biologics (blood, tissues, stem cells, cord cells) • Requirements modeling DOD using Institute of Defense Analysis (IDA) Only Government Agencies are part of this modeling effort.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED • National Infrastructure Protection Plan (2006) – Michael Chertoff, Sec DHS
Armed Services Blood Program Defense Infrastructure Sector Assurance Plan (DISAP) v. 2.1 LMI
Armed Services Blood Program DISAP Topics • National Critical Infrastructure Program • DoD Critical Infrastructure Program • DoD Health Sector CIP Program • Information Systems Support • Capability Area Working Documents • Vulnerability Assessment Protocols
Biodefense for the 21st Century: “…a blueprint for our future biodefense program…that fully integrates the sustained efforts of the national and homeland security, medical, public health, intelligence, diplomatic, and law enforcement communities.” George W. Bush April 28, 2004 • Threat Awareness / Anticipation of Future Threats • Prevention and Detection • Surveillance and Detection • Response and Recovery • Capabilities required for response based on interagency-agreed scenarios derived from plausible threat assessments • Mass Casualty Care • Risk Communication • Decontamination • MEDICAL COUNTERMEASURE DEVELOPMENT
Armed Services Blood Program ASBP - DHHS Partnership Initiatives • Blood, stem cells, tissue, and organs are a critical medical counter measure • Local planning and national participation with monitoring systems – BASIS/BRAMS • National Blood Reserve (Agree with it or not) • Frozen products as backfield • Frozen RBC • Frozen Platelets • Fresh Frozen Plasma • Hemostatic agents • Chitosan-dressing • Celox – arterial bleeding
Armed Services Blood Program ASBP - DHHS Partnership Initiatives • Efficacy studies of whole blood v. component therapy • Efficacy studies of age of blood • Rapid Testing to support initial screening “walking donors” • Hemoglobin based Oxygen Carriers (HBOC) • Novo-Seven or “cocktail” • Platelet Substitutes • Pathogen inactivation • Blood pharming - rbc and platelets
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Multiply Blood Program Offices – Lack Ability to Plan Efficiently and Execute - MTS Boxes (Logistics) • Non-FDA Licensed Blood Product Transfusions • Golden Hour Box Validations • Technology Implementation • Leuko-reduction • DBL RBC Collections • DBL Plasma Collections • RBCXL • Convalescent Plasma • Information Blood Systems • Transfusion Medicine Experts • Blood Research and Development • Managing DOD CONUS Blood Inventories
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Who Answers for the ASBP? • Secretary of Defense • Under Secretary of Defense for Personnel and Readiness • Assistant Secretary of Defense (ASD) for Health Affairs • ASD (HA) Force Health Protection and Readiness • ASD (HA) Clinical Plans and Policy ASBPO held directly accountable for events and outcomes it has no authority or control over.
Armed Services Blood Program Feb 08 (same): Command, Control, and Funding Line (Installation Commander) Service-specific Medical Service Surgeon General Health Affairs MTF CO Armed Services Blood Program Office Service Blood Program Officer Chief OIC Medical Treatment Facility FDA Licensed Program Ancillary Services JCS DHHS Blood Donation Center Blood Transfusion Center Typical reporting structure Some BDCs are stand-alone or use other staffing arrangements COCOMS • Blood Program HQ Offices has responsibility but no authority for resources • Blood donor centers compete with health care delivery for funds and staffing
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED The Transformation
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Drivers of Enterprise Transformation for the Armed Services Blood Program • Service Blood Programs operating independently, resulting in: • Operational redundancies • Disparate chains of command • Inability to generate efficient, positive change • Disparate governance and authority over policy • Disjointed and inefficient use of enterprise technology, data, and information • Objective: • Improve governance and authority of a central blood program office over ASBP organizational resources, business processes, information, and technologies • Reduce redundancies and inefficiencies which have developed over time among the Service Blood Programs • Define and implement business processes, information, data, and technology
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Transformation: Getting There Under Secretary of Defense for Personnel and Readiness or Assistant Secretary of Defense for Health Affairs, with Joint Staff concurrence, signs “directive” or charters Force Health Protection and Readiness to execute a study of the ASBP on “as is”, “what it should be”, and “how to get there.” BLUF: “The current ASBP organization must be changed based on patient safety alone.”
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Transformation Transformation concept and study implementation plan approved by: • JSC J4 (HSSD) • ASD(HA)FHP&R • OTSG (as ASBPO EA) Study is funded and pending contract execution.
Armed Services Blood Program Transformation • The study begins with meeting the needs of the stakeholders/customers: • COCOMs • JCS (J4 HSSD) • ASD(HA)FHP&RP2 • ASD(HA)CPP • Dept Homeland Defense • Dept Health and Human Services (via MOU)
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Transformation Benefits • Duplicate processes, information, data, and systems will be unified under a single ASBP Business Enterprise Architecture (BEA) • ASBP goals will be aligned with those of MHS; misalignments will be identified and resolved • All Service Blood Programs will work as a single cohesive unit, while retaining service affiliation. • ASBP goals will be aligned with those of DHHS; eliminate redundancies in R&D, improve command and control, and logistics of a national proportion.
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED Transformation Approach • Utilize the mandated and best practice Department of Defense Architecture Framework (DoDAF) • Analysis of current state ASBPO architecture (“Where we are”) • Define future state ASBPO architecture (“Where we want to be”) • Define and implement transition activities (“How we will get there”) • Identify vision of future state Concept of Operations (ConOps) • Develop operational detail of how vision will be realized in terms of organizational, management, technology governance, budget, and other terms. • Create transition plan detailing how to take ASBPO from current state to future state of operations.
Armed Services Blood Program Libby’s Transformation Future Vision • Establish one blood program agency (Defense Agency or part of JFCOM) • Single FDA License • Single Command and Control • Civilian staff – continuity of experience and knowledge • Establish a Transfusion Medicine Branch • Join with DHHS / Homeland Security – Homeland Defense • PHS Officers/staff (Indian reservations, US Territories, Prisons) • Need a National Blood Program for disaster preparedness (all countries of the world have a national program) • Veterans Affairs partnership • Oversight of tissue and organs • Cost effective
Armed Services Blood Program www.militaryblood.dod.mil UNCLASSIFIED