Download
1 / 16
210 likes | 1.13k Vues
Patient. 20 yo female presents with 3 days of fever, pleuritic chest pain, and SOBPreviously healthyNo medicationsJust started smoking last weekNo known drug or toxin exposureNo recent travel. From Pope-Harman, et al. Findings were similar on the right (sorry!). Arrows indicate Kerley B lines. .

E N D
1. Acute Eosinophilic Pneumonia Annie Weinsoft, MS4
Radiology
Spring 2007
3. Patient 20 yo female presents with 3 days of fever, pleuritic chest pain, and SOB
Previously healthy
No medications
Just started smoking last week
No known drug or toxin exposure
No recent travel
4. Patient, cont. Both CXR and CT show:
Diffuse ground glass opacities and areas of consolidation
Septal/interlobular thickening
Bilateral pleural effusions
No e/o cardiac enlargement.
CBC: Elevated WBC with left shift
Bronchoalveolar lavage:
30% Eosinophils, no e/o infection
Diagnosis?
6. Acute Eosinophilic Pneumonia (AEP) AKA Idopathic Acute Eosinophilic Pneumonia
Rare
Acute febrile illness
Tends to occur in young (ave 30 yo), previously healthy patients
Often requires mechanical ventilation
Resolves quickly with corticosteroids
Some reports of spontaneous recovery
7. AEP Criteria Acute onset of respiratory sx
< 1 month (older criteria use 7 days)
Bilateral diffuse �infiltrates� on CXR
Severe hypoxemia
PaO2 on RA < 60
PaO2/FiO2 < 300, or
Or O2 sat on RA < 90%
Lung eosinophilia (may or may not have peripheral eos, as well)
> 25% on bronchoalveolar lavage, or
Eosinophilic infiltration on lung bx (more invasive, probably unnecessary unless done for other reasons)
Absence of known cause of lung eosinophilia
Known causes include: infections, exposure to certain drugs, asthma
Patients with exposure to smoke and/or inhaled dusts are not excluded from the diagnosis
8. Eosinophilic Pneumonias AEP is within a spectrum of EP which also includes:
Loffler Syndrome / Simple EP
Chronic EP
Churg-Strauss Syndrome
Hypereosinophilic Syndrome
9. Non-idiopathic pulmonary eosinophilias Numerous other causes, including:
Parasitic infections
Ascaris, larva migrans, strongyloides, etc.
Fungal infections
Bronchopulmonary aspergillosis, etc.
Some bacterial/viral pneumonias
Toxic exposures
Local radiation therapy/exposure
Asthma
Eosinophilic bronchitis
Lung transplant
Paraneoplastic syndromes
Sarcoidosis
10. Possible associations with AEP Smoking, especially new-onset
Military study (Shorr et al) of 18 patients in Iraq found a significant increased risk with new-onset cigarette smoking within 2 weeks-2 mo of illness
Should we trust a study whose follow-up was done at Walter Reed?
Predisposition toward allergic rhinitis
82% had allergic diathesis by RAST or skin testing in study by Hayakawa
No correlation with Asthma (except in chronic EP)
Exposure to inhaled dusts and/or other noxious substances
No increased risk in military study, but other case series have noted several patients with recent exposures to substaces such as dust, smoke, wood particles, and/or tear gas. Significance of these exposures is unclear.
11. Typical Appearance on Chest CT
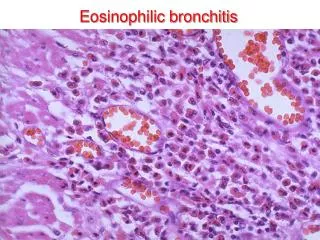
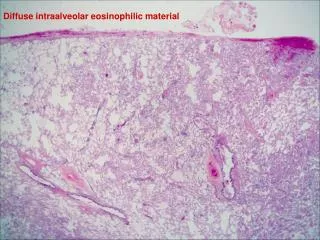
12. AEP Histologic Appearance Above (Pope-Harman): Septal edema, fluid in alveoli, eosinophis and macrophages infiltrating both septa and alveoli.
Right (Mochimaru): Intra-alveolar fibrin deposition
13. So, how do we recognize AEP? Consider it if you see:
Severe, acute febrile pneumonia with radiographic appearance of hydrostatic/permeability edema
Check lavage fluid for eosinophilia
Rule out other causes (when reasonable)
Unexpected eosinophilia on CBC, bronchoalveolar lavage, and/or lung biopsy
Chararteristic history, such as new-onset cigarette smoking
14. Treatment Most cases are non-fatal, with appropriate supportive care
Recovery typically occurs in 1-2 weeks, with no recurrences
Traditional treatment has been with systemic corticosteroids (no exact regimen established)
Several reports of patients recovering spontaneously without steroids, though this remains somewhat controversial.
15. The End
16. References Cottin V, Cortier JF. Eosinophilic Pneumonias. Allergy 2005;60:841
Mochimaru H, et al. Clinicopathological differences between acute and chronic eosinophilic pneumonia. Respirology 2005;10:76
Pope-Harman AL, et al. Acute eosinophilic pneumonia: a summary of 15 cases and review of the literature. Medicine (Baltimore) 1996;75(6):334
Philit F, et al. Idopathic acute eosinophilic pneumonia: a study of 22 patients. Am J Respir Crit Care Med 2002;166:1235
Hayakawa H, et al. A clinical study of idopathic eosinophilic pneumonia. Chest 1994;105:1462
Kim Y, et al. The spectrum of eosinophilic lung disease: radiographic findings. J Comput Assist Tomogr 1997;21(6):920
Shorr AF, et al. Acute eosinophilic pneumonia among US military personnel deployed in or near Iraq. JAMA 2004;292:2997
Ketai LH, Godwin JD. A new view of pulmonary edema and acute respiratory distress syndrome. J Thorac Imaging 1998;13:147