Download
1 / 9
90 likes | 214 Vues
Introduction. Results. Conclusions. Method. Anxiety Sensitivity and Contextual Cues as Predictors of Fearful Responding to Inhalation of CO 2 : Testing their Interaction in a Sample without a History of Panic. Jasper A.J. Smits, Mandy Dement, Mark B. Powers, Hanjoo Lee, & Michael J. Telch.

E N D
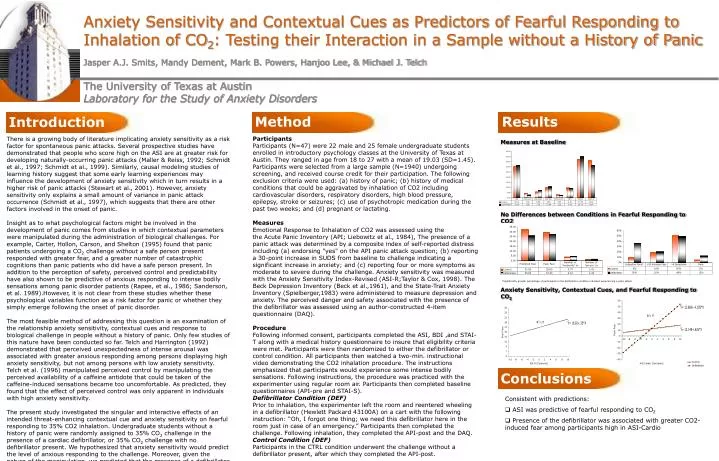
Introduction Results Conclusions Method Anxiety Sensitivity and Contextual Cues as Predictors of Fearful Responding to Inhalation of CO2: Testing their Interaction in a Sample without a History of Panic Jasper A.J. Smits, Mandy Dement, Mark B. Powers, Hanjoo Lee, & Michael J. Telch The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Participants Participants (N=47) were 22 male and 25 female undergraduate students enrolled in introductory psychology classes at the University of Texas at Austin. They ranged in age from 18 to 27 with a mean of 19.03 (SD=1.45). Participants were selected from a large sample (N=1940) undergoing screening, and received course credit for their participation. The following exclusion criteria were used: (a) history of panic; (b) history of medical conditions that could be aggravated by inhalation of CO2 including cardiovascular disorders, respiratory disorders, high blood pressure, epilepsy, stroke or seizures; (c) use of psychotropic medication during the past two weeks; and (d) pregnant or lactating. Measures Emotional Response to Inhalation of CO2 was assessed using the the Acute Panic Inventory (API; Liebowitz et al., 1984), The presence of a panic attack was determined by a composite index of self-reported distress including (a) endorsing "yes" on the API panic attack question; (b) reporting a 30-point increase in SUDS from baseline to challenge indicating a significant increase in anxiety; and (c) reporting four or more symptoms as moderate to severe during the challenge. Anxiety sensitivity was measured with the Anxiety Sensitivity Index-Revised (ASI-R;Taylor & Cox, 1998). The Beck Depression Inventory (Beck et al.,1961), and the State-Trait Anxiety Inventory (Spielberger,1983) were administered to measure depression and anxiety. The perceived danger and safety associated with the presence of the defibrillator was assessed using an author-constructed 4-item questionnaire (DAQ). Procedure Following informed consent, participants completed the ASI, BDI ,and STAI-T along with a medical history questionnaire to insure that eligibility criteria were met. Participants were then randomized to either the defibrillator or control condition. All participants then watched a two-min. instructional video demonstrating the CO2 inhalation procedure. The instructions emphasized that participants would experience some intense bodily sensations. Following instructions, the procedure was practiced with the experimenter using regular room air. Participants then completed baseline questionnaires (API-pre and STAI-S). Defibrillator Condition (DEF) Prior to inhalation, the experimenter left the room and reentered wheeling in a defibrillator (Hewlett Packard 43100A) on a cart with the following instruction: “Oh, I forgot one thing; we need this defibrillator here in the room just in case of an emergency.” Participants then completed the challenge. Following inhalation, they completed the API-post and the DAQ. Control Condition (DEF) Participants in the CTRL condition underwent the challenge without a defibrillator present, after which they completed the API-post. There is a growing body of literature implicating anxiety sensitivity as a risk factor for spontaneous panic attacks. Several prospective studies have demonstrated that people who score high on the ASI are at greater risk for developing naturally-occurring panic attacks (Maller & Reiss, 1992; Schmidt et al., 1997; Schmidt et al., 1999). Similarly, causal modeling studies of learning history suggest that some early learning experiences may influence the development of anxiety sensitivity which in turn results in a higher risk of panic attacks (Stewart et al., 2001). However, anxiety sensitivity only explains a small amount of variance in panic attack occurrence (Schmidt et al., 1997), which suggests that there are other factors involved in the onset of panic. Insight as to what psychological factors might be involved in the development of panic comes from studies in which contextual parameters were manipulated during the administration of biological challenges. For example, Carter, Hollon, Carson, and Shelton (1995) found that panic patients undergoing a CO2 challenge without a safe person present responded with greater fear, and a greater number of catastrophic cognitions than panic patients who did have a safe person present. In addition to the perception of safety, perceived control and predictability have also shown to be predictive of anxious responding to intense bodily sensations among panic disorder patients (Rapee, et al., 1986; Sanderson, et al. 1989).However, it is not clear from these studies whether these psychological variables function as a risk factor for panic or whether they simply emerge following the onset of panic disorder. The most feasible method of addressing this question is an examination of the relationship anxiety sensitivity, contextual cues and response to biological challenge in people without a history of panic. Only few studies of this nature have been conducted so far. Telch and Harrington (1992) demonstrated that perceived unexpectedness of intense arousal was associated with greater anxious responding among persons displaying high anxiety sensitivity, but not among persons with low anxiety sensitivity. Telch et al. (1996) manipulated perceived control by manipulating the perceived availability of a caffeine antidote that could be taken of the caffeine-induced sensations became too uncomfortable. As predicted, they found that the effect of perceived control was only apparent in individuals with high anxiety sensitivity. The present study investigated the singular and interactive effects of an intended threat-enhancing contextual cue and anxiety sensitivity on fearful responding to 35% CO2 inhalation. Undergraduate students without a history of panic were randomly assigned to 35% CO2 challenge in the presence of a cardiac defibrillator, or 35% CO2 challenge with no defibrillator present. We hypothesized that anxiety sensitivity would predict the level of anxious responding to the challenge. Moreover, given the nature of the manipulation, we predicted that the presence of a defibrillator would only lead to increased anxious responding among participants reporting high cardiovascular sensitivity. Measures at Baseline No Differences between Conditions in Fearful Responding to CO2 *Significantly greater percentage of participants in the defibrillator condition indicated experiencing a panic attack. Anxiety Sensitivity, Contextual Cues, and Fearful Responding to CO2 • Consistent with predictions: • ASI was predictive of fearful responding to CO2 • Presence of the defibrillator was associated with greater CO2-induced fear among participants high in ASI-Cardio
Introduction Results Conclusions Method THE UNIVERSITY OF TEXAS AT AUSTIN LABORATORY FOR THE STUDY OF ANXIETY DISORDERS Thought-Action Fusion and Its Relationship to Schizotypy and OC Symptoms Han-Joo Lee, MA, Jesse R. Cougle, MA, & Michael J. Telch, PhD MeasuresThe Thought-Action Fusion Scale-Revised (TAFS; Shafran et al., 1996). Schizotypal Personality Scale (STA; Claridge & Broks, 1984). This a 37-item self-report measure of schizotypal personality traits, assessing 3 robust factors: (a) magical thinking, (b) unusual perceptual experiences, and (c) paranoid ideation. State-Trait Anxiety Inventory – Trait version (STAI; Speilberger et al., 1983). Beck Depression Inventory - II (BDI-II; Beck, Steer, & Brown, 1996). Obsessive Compulsive Inventory-Revised (OCI-R; Foa et al., 2002). 3. Predicting OC Symptoms with Schizotypal Traits Step 1:the BDI and STAI-T (R2 = .160, F = 91.82, p < .001) Step 2: the three STA subscales (D R2 = .083, F = 35.32, p < .001) significantly predicted OC symptoms (8.3% of the variance in OC symptoms). After Controlling for Likelihood TAF Step 1:the BDI and STAI-T Step 2: Likelihood TAF Step 3: the three STA subscales (DR2 = .062, F = 27.03, p < .001) The magical thinking subscale was no longer significant after likelihood TAF was controlled, whereas the other two STA subscales were still significant predictors. After Controlling for Moral TAF Step 1:the BDI and STAI-T Step 2: Moral TAF Step 3: the three STA subscales (D R2 = .080, F = 34.35, p < .001) All the STA subscales remained significant predictors. Thought-action fusion (TAF) refers to a set of cognitive biases involving faulty causal relationships between one’s own thoughts and external reality (Shafran, Thordarson, & Rachman, 1996). Moral TAF is the belief that having unacceptable thoughts is as bad as actually carrying them out. Likelihood TAF is the belief that having an unacceptable or disturbing thought will increase the likelihood that the thought will occur in reality. It is possible that likelihood-TAF is an extreme cognitive bias associated with magical thinking and schizotypal traits; whereas moral TAF is common among those adhering to a strict moral code, and therefore less associated with OCD symptoms and extreme magical thinking. To date, several findings appear to provide indirect support for this hypothesis: (a) elevated moral TAF is frequently observed among nonclinical populations, whereas likelihood TAF is not (Shafran et al., 1996); (b) nonclinical subjects and OCD patients do not differ with respect to moral TAF but OCD patients score significantly higher than nonclinical subjects on likelihood TAF (Rassin, Merckelbach, Muris, & Schmidt, 2001); (c) likelihood TAF is more strongly associated with OCD symptoms relative to moral TAF (Amir et al, 2001; Coles et al., 2001). Finally, unlike moral TAF, likelihood TAF is positively associated with indices of anxiety and worry (Hazlett-Stevens, Zucker, & Craske, 2002). Despite evidence suggesting that OCD and schizophrenia are distinguishable, there is a line of research suggesting a possible linkage between OCD and schizotypy. About half of OCD patients exhibit mild to severe levels of schizotypal traits, which may suggest the existence of a schizotypy subtype of OCD (Sobin et al., 2000). Interestingly, OCD patients appear to be indistinguishable from schizophrenic patients and bipolar patients with respect to schizotypy, although all three groups score higher than unipolar depressive patients (Rossi & Daneluzzo, 2002). This study sought to investigate the possible connection between the two types of TAF, schizotypy traits, and OCD symptoms using a nonclinical student sample. We hypothesized that likelihood TAF will be more strongly associated with schizotypal traits (especially magical thinking), and that the relationship between likelihood TAF and OCD symptom severity will in part be explained by the association between likelihood TAF and schizotypal traits. Table 1. Zero-order Correlations between the Study Measures Our findings provide preliminary evidence for a positive association between likelihood TAF and schizotypal traits. Moral TAF showed no relationship with schizotypy and was only weakly associated with OCD symptoms, depression, and anxiety. The magical thinking facet of schizotypy may put one at greater risk for displaying the cognitive bias of likelihood TAF, which in turn may increase one’s risk for OCD. Several findings from the present study are consistent with this hypothesis: (a) a significant positive association was found between the magical thinking subscale of the STA and OCD symptoms; (b) the relationship between magical thinking and likelihood TAF was also significant; and (c) most importantly, the relationship between the magical thinking subscale of the STA and OCD symptoms was no longer significant after controlling for likelihood TAF. * p<.05 ** p<.01 TAF-M=Moral TAF; TAF-L=Likelihood TAF; STA=Schizotypal personality scale; STA-M=Magical thinking; STA-U=Unusual perceptual experiences; STA-P=Paranoid ideation Hierarchical Regression Analyses 1. Predicting TAF with Schizotypal Traits In Predicting Likelihood TAF Step 1: the BDI, STAI-T, and OCI (R2 = .138, F = 51.39, p < .001) Step 2: the three STA subscales (D R2 = .072, F = 29.29, p < .001) Magical Thinking was the only significant predictor(b = .30, t = 8.45, p <.001). In Predicting Moral TAF Step 1:the BDI, STAI-T, and OCI (R2 = .020, F = 6.69, p < .001) Step 2: the three STA subscales (DR2 = .003, F = .85, p = .468) None of the STA subscales predicted moral TAF. 2. Predicting OC Symptoms with TAF Step 1:the BDI and STAI-T (R2 = .160, F = 91.82, p < .001) Step 2: Likelihood TAF (DR2 = .042, F = 50.55, p < .001) or Step 2: Moral TAF (D R2 = .013, F = 15.02, p < .001) Controlling for Schizotypal Traits Step 1: the BDI and STAI-T Step 2: the three STA subscales Step 3: Likelihood TAF (DR2 = .021, F = 26.91, p < .001) or Step 3: Moral TAF (DR2 = .01, F = 12.39, p < .001) Likelihood TAF (4.2% 2.1%); Moral TAF (1.3% 1.0%) LikelihoodTAF SchizotypyMagical Thinking ObsessiveCompulsive Symptoms Participants Nine hundred sixty-eight undergraduate students (659 women and 309 men) enrolled in introductory psychology classes at the University of Texas at Austin. Figure 1. Hypothesized relationship between schizotypy-magical thinking, Likelihood TAF and OCD symptoms
THE UNIVERSITY OF TEXAS AT AUSTIN LABORATORY FOR THE STUDY OF ANXIETY DISORDERS A Comparison of Autogenous/Reactive Obsessions and Worry in a Nonclinical Population Han-Joo Lee, MA1, Soon-Hee Lee, MA2, Hyang-Suk Kim, MA2, Seok-Man Kwon, PhD2, & Michael J. Telch, PhD11 University of Texas at Austin, 2 Seoul National University, Seoul, South Korea Introduction Thought Content Appraisals Participants 435 undergraduate students (317 women and 118 men) enrolled in introductory psychology classes at the University of Texas at Austin Measures Revised Obsessional Intrusion Inventory (ROII; Purdon & Clark, 1993). The ROII Part I assesses 52 intrusive thoughts and Part II further evaluates the most distressing thought selected from Part I. Lee and Kwon (2003) proposed two distinctive subfactors of Part I: autogenous obsessions, which include sexual, aggressive, or blasphemous thoughts, and reactive obsessions, which include thoughts about mistakes, accidents, or contamination. Subscale frequency scores were computed separately for autogenous and reactive obsessions. Worry Domain Questionnaire Short form(WDQ-SF;Stöber and Joormann, 2001).The WDQ assesses the amount of worry across five domains of everyday concern: relationships, lack of confidence, aimless future, work, and financial issues. Thought Examination Scale (TES).The TES contains 13 statements constructed by the authors to examine various thought characteristics of obsessions and worry. Participants rate to what extent they agree on each statement with respect to their most distressing thought (0=Not at all~4=Absolutely). 13 items formed 3 domains: (a) Thought Content Appraisal (i.e., The content of this thought is bizarre/ reflects worry about real-life problems/ is very unacceptable/ is realistic/ is likely to come true); (b) Thought Form Perception [i.e., This thought takes the form of an impulse(s) or urge(s)/ image(s)/ thought(s)/ doubt(s) or apprehension(s)]; (c) Thought Trigger Perception (i.e., When this thought occurs, I can recognize some specific triggers that evoked it; This thought pops into my mind without any triggers; This thought is evoked by apprehension about some future event; I clearly know what evokes this thought). Beck Depression Inventory-II / State-Trait Anxiety Inventory – Trait (STAI-T) Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990) Obsessive Compulsive Inventory – Revised (OCI-R; Foa et al., 2002) Thought Control Questionnaire (TCQ; Wells & Davies, 1994). The TCQ consists of 5 subscales: distraction, social coping, worrying, punishment, and re-appraisal. Procedures Based on the most distressing thought, participants were classified into three subgroups (AO vs. RO vs. WO) and compared. Bizarre Real-life Problems Unacceptable Realistic Likely to come true Several authors have documented differences between obsessions and worry. Relative to obsessions, worry is more ego-syntonic and less intrusive, being evoked by more identifiable triggers (Turner, Beidel, & Stanley, 1992). Worry was also found to be rated as more verbally oriented, more realistic, longer in duration, more distracting, less dismissible and more often associated with a greater compulsion, compared to obsessions (Wells & Morrison, 1994). Recently, an obsession model has been proposed (Lee & Kwon, 2003), presenting two different subtypes. Autogenous obsessions (AOs) include sexual, aggressive, blasphemous or repulsive thoughts, images, or impulses. They tend to be perceived as very ego-dystonic and unacceptable, and evoke efforts to remove or control the thought(s) themselves. Moreover, they are likely to be elicited without clear triggers or by some triggers symbolically or remotely associated with the thoughts (e.g., the alphabet S triggering the thought of killing one's sister). Reactive obsessions (ROs) include thoughts, concerns, or doubts about contamination, mistakes, accidents, asymmetry or disarray. They tend to be perceived as relatively realistic and likely to come true, and elicit overt actions aimed at putting the associated uncomfortable situation back to a safe or desired state. Moreover, they are likely to be triggered primarily by external cues, which correspond to specific core threats (e.g., exposure to dirt activating the threat of contamination, which is neutralized through washing rituals). We hypothesized that, compared to AOs, ROs would be more similar to worry. In other words, they may form a continuum on several thought characteristics, with ROs falling in between AOs and worry (See Figure 1). AO RO WO AO RO WO AO RO WO AO RO WO AO RO WO (* p<.01 by Bonferoni correction) Thought Form Perceptions Impulse/Urge Doubt/Apprehen. Images Thoughts AO RO WO AO RO WO AO RO WO AO RO WO (* p<.02 by Bonferoni correction) Thought Trigger PerceptionsTCQ Can recognize Triggered by other Clearly know what Worrying triggers apprehensions evokes the thought Strategy e.g., ‘I left the door unlocked!’ ‘I am contaminated. I’ll get sick’ ReactiveObsessions Results AO RO WO AO RO WO AO RO WO AO RO WO e.g., ‘Have sex with my father!’ ‘Kill my sister!’ e.g., ‘What if I fail in the coming exam?’/ ‘I will lose my job…’ Zero-order Correlations among Study Measures AutogenousObsessions - ROII-A: Autogenous Obsessions- ROII-R: Reactive Obsessions- Partial correlations controlling for the BDI and STAI are presented in gray. * p<.05 ** p<.01 *** p<.001 Compared to autogenous obsessions, Reaction obsessions revealed significantly higher correlations with severity of worry as measured by both the WDQ and the PSWQ (p<.01 using Fisher-Z transformation). Worry (* p<.02 by Bonferoni correction) Compared to ROs, AOs are more similar to worry. Our findings are in line with previous findings highlighting the differences between worry and obsessions (Langlois et al., 2000; Wells & Morrison, 1994; Turner et al., 1992), replicating some of the major findings that worry was more realistic, less ego-dystonic, more persistent, more verbally oriented compared to obsessions. However, our findings also suggest that the differences between worries and AOs are more striking than the differences between worries and ROs. Figure 1. A hypothesized continuum of autogenous obsessions, reactive obsessions, and worry
Introduction Results Method THE UNIVERSITY OF TEXAS AT AUSTIN LABORATORY FOR THE STUDY OF ANXIETY DISORDERS Testing the Autogenous-Reactive Model of Obsessions Han-Joo Lee, MA1, Seok-Man Kwon, PhD2, Jun Soo Kwon, MD, PhD3, & Michael J. Telch, PhD1 1University of Texas at Austin, 2Seoul National University, Seoul, South Korea, 3Seoul National University Hospital, Seoul, South Korea Recently, an obsession model has been proposed which classifies obsessions into two subtypes (Lee & Kwon, 2003). Participants Twenty-seven patients diagnosed as OCD based on the Structured Clinical Interview for DSM-IV (First et al, 1996) were recruited from the OCD outpatient clinic at Seoul National University Hospital. They were negative for bipolar disorder, schizophrenia, and substance abuse. They consisted of 21 men and 6 women ranging in age from 17 to 56 (M = 28.96; SD =9.18). Measures Maudsley Obsessional-Compulsive Inventory (MOCI; Hodgson & Rachman, 1977). This OC symptom measure comprises five subscales: Checking, Washing, Slowness, Doubting, and Rumination. Padua Inventory(PI; Sanavio, 1988). This is a 60-item self-report measure of OC symptoms consisting of four sub-factors: (a) Impaired Control over Mental Activities, (b) Becoming Contaminated, (c) Checking Behavior, and (d) Urges and Worries of Losing Control of Motor Behavior. Obsessional Belief Questionnaire(OBQ; OCCWG, 2001).This a 87-item self-report measure assessing dysfunctional beliefs relevant to OCD, consisting of six sub-scales: (a) Inflated Responsibility, (b) Overimportance of Thoughts, (c) Control of Thoughts, (d) Overestimation of Threat, (e) Intolerance of Uncertainty, and (f) Perfectionism. Multidimensional Perfectionism Scale (MPS: Frost et al., 1990). This is a 35-item self-report measure of perfectionistic personality features, consisting of six subscales: (a) Concern Over Mistakes, (b) Personal Standards, (c) Parental Expectations, (d) Parental Criticism, (e) Doubts about Actions, and (f) Organization. OCD Patients Subgrouping Procedure Participants reported their most distressing obsessions up to three, and the primary obsession for each patient was determined based on a two-fold criterion that required the obsession to be reported as both the most upsetting and the most frequent. Three master’s level clinical psychologists independently classified the primary obsessions as either autogenous or reactive based on their content. Consistent with the model of Lee and Kwon (2003), obsessions were classified as falling in the autogenous subtype if they dealt with sexual, violent, aggressive, blasphemous, or repulsive thoughts, images, or impulses. In contrast, concerns, doubts, or worries about mistakes, contamination, disorder, or disarrangement were classified as obsessions falling into the reactive subtype. The mean inter-rater reliability using Kappa index (Siegel & Castellan Jr, 1988) was .95. Based on this procedure, each participant was classified as having an autogenous obsession (autogenous patients; N = 13) or a reactive obsession (reactive patients; N = 14) as primary. Autogenous and reactive patients did not differ significantly on severity of depression, anxiety, as well as OC symptom (as measured by the PI). Differences in OCD Symptoms, Perfectionistic Personality Features, and Dysfunctional Beliefs between Autogenous and Reactive Patients Autogenous obsessions were rated as more dislikable and guilt-provoking, whereas reactive obsessions evoked greater worries that the thought might come true. Autogenous obsessions were also perceived as more unacceptable or threatening to merely have in mind, whereas reactive obsessions were perceived as more realistic and evoked a greater sense of personal responsibility to prevent harm. Moreover, autogenous obsessions elicited more avoidant thought control strategies, whereas reactive obsessions elicited more confrontational, behavioral control strategies (Lee & Kwon, 2003; Lee, Kwon, Kwon, & Telch, 2003). This study classified OCD patients as displaying either autogenous or reactive as their primary obsession and then compared with respect to several OCD-related domains, including OC symptom profiles, perfectionistic personality features, and dysfunctional beliefs. More specifically, (a)autogenous patients would be more apt to display obsessional, ideational, or covert symptoms; whereas reactive patients would be more apt to display overt, behavioral symptoms; (b) We also predicted that reactive patients would demonstrate the often observed perfectionistic personality features associated with OCD (Frost & Steketee, 1997), whereas autogenous patients would display lower levels of perfectionism. This was based on the clinical observation that reactive patients often display exceedingly high and rigid standards and strive harder to organize and control their environments in order to ensure that they are not in unsafe or undesired situations; and (c)Compared to autogenous patients, reactive patients would score higher on the belief domains of Inflated Responsibility, Threat Overestimation, Perfectionism, and Intolerance of Uncertainty as measured by the OBQ, since these beliefs may heighten sensitivity to possible harm and perceived responsibility associated with their obsessions. * p<.05 ** p<.01 Preliminary findings in support of two distinct OCD subtypes based on the autogenous-reactive classification: Reactive patients displayer more overt OC symptoms and greater perfectionistic tendencies than autogenous patients. Moreover, inflated responsibility, intolerance of uncertainty, and perfectionistic beliefs were more prominent in reactive patients relative to autogenous patients. The manifestation of autogenous obsessions may be more linked to impaired control over one’s thoughts and impulses, whereas reactive obsessions are more related to excessive urges and need for control over one’s environment. It has also been demonstrated that, compared to reactive obsessions, autogenous obsessions were more strongly associated with schizotypal traits (i.e., magical thinking, unusual perceptual experiences) and thought disorder tendencies (Lee, Kwon, Kwon, & Telch, 2003; Lee, Kim, & Kwon, 2003).
Abstract Results Conclusions Introduction Method Active-Imaginal Exposure: Examination of a New Behavioral Treatment for Cynophobia (Dog Phobia) Mark B Powers, Timothy O. Rentz , Jasper A.J. Smits, Jesse Cougle, & Michael Telch The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Response rates at posttreatment and follow-up as a function of treatment condition. The aims of this study were to investigate exposure-based treatments for cynophobia (dog phobia) and to test a newly developed hybrid imaginal exposure treatment that we have named active imaginal exposure. The treatment introduces an in vivo coping component to imaginal exposure whereby the patient physically performs coping responses to an imagined feared stimulus. Eighty-two participants meeting DSM-IV criteria for specific phobia (animal subtype) were randomly assigned to one of three 30-min. treatments: (a) active-imaginal exposure (AI), b) imaginal exposure alone (IE), or (c) graduated in-vivo exposure (IV). Participants completed a behavioral approach test at pre, post, and four-week follow-up. Significant pre- to posttreatment improvement was observed in all three treatment conditions. Response rates at posttreatment were 51.9%, 62.1%, and 73.1% for the IE, AI, and IV groups respectively. Likewise, effect sizes at posttreatment were .76, 1.41, and 1.55 for the IE, AI, and IV groups respectively. Although in the predicted direction, the between group differences were not significant. A similar pattern of results was observed at follow-up. Further, safety behavior utilization during treatment was associated with less improvement – particularly in the two imaginal treatment conditions. Exposure treatments of dog phobia appear feasible and effective in reducing phobic fear and avoidance associated with dog phobia. Furthermore, preliminary evidence suggests that our active-imaginal exposure treatment may be a viable alternative to in vivo exposure. Participants Eighty-two participants meeting DSM-IV criteria for specific phobia, animal type, took part in the experiment. Participants were recruited from the undergraduate introductory psychology subject pool at the University of Texas at Austin, and from the Austin community. The final sample was predominately female (87.8%) and ethnically diverse (Black=24.4%, White=22.0%, Hispanic=22.0%, Asian=31.7%, American Indian=1.2%). Mean age of the sample was 18.9 years (SD=3.7). Students received partial course credit for their participation. Measures Diagnostic Interview Composite International Diagnostic Interview (CIDI) (World Health Organization, 1997) Outcome Measures Peak Subjective Fear Number of BAT Steps Completed Reliable Change and High End State Functioning (Jacobson and Truax, 1991) Relapse: Relapse was defined as a reliable posttreatment to follow-up increase in fear or decrease in approach. Treatment Conditions In vivo Exposure (IV). Participants assigned to the IV condition approached and handled two real dogs on leashes, one at a time for 15 minutes each, in a quiet, distraction free hallway, for a total of 30 min., excluding time between trials. At approximately 30 sec. intervals, participants were cued to state aloud their current fear level as they repeatedly performed each task in the hierarchy with the real dog. Each treatment step was terminated when the participant's fear decreased to a SUDS level of 30 or below. At each step of the hierarchy, participants rated the dog's behaviors as threatening, submissive, or playful based on the education presented earlier. These data were later used for yoking purposes. Imaginal Exposure (IE). Participants assigned to the IE condition were shown a picture of the dog they were to imagine, which was the same dog used in the IV condition. This procedure served to maintain consistency in dog stimuli across the three conditions. Participants were seated in a quiet room with their eyes closed, and imagined themselves performing the hierarchy steps according to a script read by the experimenter. The script described the tasks, which were identical for all groups, as well as the appearance and behavior of the dog, which was yoked to reports of the dog’s behavior made by participants in the in vivo condition. After imagining each task in the hierarchy, participants were instructed to open their eyes and turn their attention to the experimenter, who then recorded the process data described above, as well as the participants’ ratings of image clarity on a 0 (no image present) to 100 (perfectly clear) scale. Active-Imaginal Exposure (AI) Participants assigned to the AI condition were shown a picture of the dog that they were to imagine, which was the same dog used in the IV condition. While imagining the dog, participants physically performed the tasks in the therapy trials according to a script read by the experimenter. The script described the tasks, which were identical for all groups, as well as the appearance and behavior of the dog, which was based on a participant’s observation of the dog’s behavior and appearance in the in vivo condition. This was the same script used in the IE condition, except that the participants physically performed the tasks and physically interacted with the imaginary dog. All process measures were collected in the same manner as in the IE condition. In order to assure the greatest possible treatment integrity, all procedures were fully manualized and administered by trained experimenters. Percent participants achieving high end state function at posttreatment and follow-up as a function of treatment condition. Regression Lines of Posttreatment Peak Fear on Safety Behavior Use Ideally, exposure-based treatments should be both powerful and convenient. Thus, researchers interested in pushing the envelope on phobia treatments are faced with the decision to either develop ways to make in vivo exposure more palatable to patients and more convenient for clinicians or to develop more potent imaginal techniques. Evidence from several sources suggests that imaginal exposure to fear-provoking cues may be enhanced through the inclusion of coping scripts into the imagery scenes. In one variation called covert modeling, the patient imagines a person modeling coping behavior in the fearful situation. Kazdin (1979) found that imaginal exposure was more effective in helping patients increase assertive behavior when they were instructed to imagine an assertive model. Similarly, Foa (1997) showed that covert modeling was an effective addition to stress inoculation training in the treatment of posttraumatic stress disorder (PTSD). The utility of integrating coping imagery into imaginal exposure to fear cues has also been demonstrated in the treatment of panic disorder (Clum, Watkins, Borden, Broyles & Hayes, 1993). In addition, Goldfried and his colleagues have shown promising results integrating imaginal coping strategies with desensitization (Goldfried, 1971; Kanter & Goldfried, 1979). The primary aim of the current study was to determine whether dog phobia could be successfully ameliorated with psychosocial treatment. A secondary aim was to test the relative efficacy of our hybrid active-imaginal treatment relative to imaginal exposure alone and the gold standard - graduated in vivo exposure. Finally, based on recent findings demonstrating that safety behavior use during exposure has a deleterious effect on treatment outcome in claustrophobia (Sloan & Telch, 2002), we examined whether safety behavior use during treatment was associated with treatment outcome. We hypothesized that all three treatments would result in clinically significant improvement in subjective fear and behavioral approach and that our hybrid active-imaginal exposure treatment would outperform imaginal exposure alone. We also predicted that safety behavior utilization during treatment would be associated with a poorer outcome at posttreatment and follow-up. • Our findings provide important data that those suffering from significant fear of dogs can be successfully treated with a brief intervention consisting of education and brief exposure-based interventions. • It also appears that active-imaginal exposure may prove to be a viable alternative to in-vivo exposure with significant practical advantages and no significant reduction in treatment efficacy. • The treatments were statistically equivalent, although there was a trend suggesting that active-imaginal exposure was more effective than imaginal exposure alone.
Introduction Results Conclusions Method Facilitating Public Speaking Fear Reduction by Increasing the Salience of Disconfirmatory Evidence: Work in Progress Jasper A.J. Smits*, Mark B. Powers, Mark Wimmer, Stacy K. Roddy, Yongrae Cho, & Michael J. Telch The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Participants: Introductory students and outpatient volunteers (N=46) meeting DSM-IV criteria for social phobia as their principal Axis I disorder, and reporting a significant fear of public speaking. Design: Eligible participants were randomly assigned to one of four treatment conditions: (a) Exposure to public speaking without feedback (EO), (b) Exposure to public speaking plus Videotape Feedback focusing on the speaker’s performance (EVS); (c) Exposure to public speaking plus Videotape Feedback focusing on the audience reaction (EVA); or (d) Credible Placebo consisting of pulsed audio/photic stimulation (D.A.V.I.D.). Treatment: All participants assigned to exposure conditions received a total of 45 min. of in vivo exposure to public speaking. The exposure was divided into five, 3-min. speech trials, across three treatment sessions. Treatment was completed in a one-week period. Participants in the feedback conditions were be told that the feedback was designed to help examine their performance more objectively and thus help lessen the original concerns about appearing weird or overly uncomfortable. Participants assigned to the placebo condition received a total of 45 min. of pulsed audio and photic stimulation along with instructions emphasizing the beneficial effects of this procedure on social anxiety. Assessment: Outcome assessments consisted of self-report questionnaires and subjective, responses during a 3-minute speech task. These measures were collected at pretreatment, and posttreatment. Social phobia is the most prevalent of all anxiety disorders (Kessler et al., 1994) and is associated with significant impairment in work and social functioning. Moreover, social phobia sufferers often develop additional psychological sequalae such as substance abuse and depression. Numerous clinical trials have demonstrated the efficacy of Cognitive Behavioral Treatment (CBT) in treating social phobia (cf. Gould, Buckminster, Pollack, Otto, & Liang, 1997). However, approximately 25% of social anxiety patients do not benefit (Heimberg et al., 1998) and of those who do benefit, most continue to display residual symptoms and impaired work/academic impairment. Consequently, there is a considerable need for developing more potent psychological treatments for social phobia. Preliminary data suggest that the provision of videotape feedback following a speech may enhance speech anxiety reduction. Rapee & Hayman, (1996) compared performance ratings of participants who received videotape feedback following a speech to performance ratings of participants who did not receive videotape feedback. The results showed a greater discrepancy between self-ratings and ratings made by independent observers among those who did not receive feedback, compared to participants who watched their speech on tape. The findings are consistent with the idea that feedback provides disconfirmatory evidence, and thereby correct the distorted perceptions. In a follow-up study, Harvey, Clark, Ehlers, and Rapee (2000) examined whether cognitive preparation would increase the beneficial effects of videotape feedback. Participants who received cognitive preparation rated their performance higher compared to those who were not given cognitive preparation. These results suggest that the beneficial effects of video feedback may be increased when the client carefully examines the discrepancy between imagined performance and actual performance. The current study examined whether cognitive-behavioral treatment for public speaking anxiety, the most common feared situation reported among social phobic sufferers (Schneier, Johnson, Hornig, Liebowitz, & Weissman, 1992), can be enhanced through the addition of videotape feedback procedures. In addition to investigating the effects of videotape feedback where the participant receives information regarding his/her performance, the current study will examine the effects of feedback of external stimuli through videotape feedback where the camera is focused on the audience. This form of feedback is hypothesized to address the overestimation of cost, as the participant receives the message that exhibiting anxiety and evaluation are not associated with disastrous consequences. In addition, instructing the participant to focus on external stimuli rather than on the self has been shown to increase the effects of exposure (Wells & Papergeorgiou, 1998). On the other hand, videotape feedback targeting the performance of the speaker is hypothesized to address the probability bias, since participants will come to see that they perform better than predicted. Outcome and Cognitive Measures at Pre- and Posttreatment Placebo-Controlled Effect Sizes for Major Outcome Measures Placebo-Controlled Effect Sizes for Cognitive Measures • Exposure treatment appears to outperform placebo; • Performance feedback appears to enhance the effects of exposure; • Audience feedback appears to reduce the potency of exposure. *This research was supported in part by a Society for a Science of Clinical Psychology Dissertation Grant awarded to Jasper A.J. Smits
Exposure Condition ______________________________________________________________ Threat Word Neutral Word Seashore Rhythm Exposure Only (Activation) Control (Distraction) Control ______________________________________________________________________________ Measure M SD M SD M SD M SD ______________________________________________________________________________ Treatment Block 1 59.1 18.2 51.2 25.0 51.4 19.7 56.5 16.6 2 58.7 19.9 41.2 23.2 48.7 18.1 41.0 23.9 3 50.7 21.5 36.7 21.4 39.0 21.1 33.3 22.9 4 38.0 18.2 28.3 18.1 33.7 19.5 24.7 21.3 5 29.3 20.5 21.0 15.8 28.0 17.3 18.7 20.7 6 25.3 21.3 15.3 16.1 22.7 18.5 12.0 15.7 _____________________________________________________________________ Growth Curve Parameters Initial Fear Activation 62.7 18.0 50.0 25.1 54.4 20.9 52.3 21.5 Between-Trial Fear Decline -7.7 4.6 -7.1 4.6 -6.0 3.0 -8.5 4.6 _____________ Note: Each treatment block consisted of five min. of exposure to the test chamber. Abstract Results Conclusions Method Fear Activation and Distraction during the Emotional Processing of Claustrophobic Fear Mark B. Powers, Jasper A.J. Smits, David P. Valentiner, Doron Ilai, Paula R. Young, & Michael J. Telch The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Primary Outcome Measures and Growth Curve Analyses Exposure Conditions ______________________________________________________________ Threat Word Neutral Word Seashore Rhythm Exposure Only (Activation) Control (Distraction) Control ______________________________________________________________________________ Measure M SD M SD M SD M SD ______________________________________________________________________________ Treatment Block 1 59.1 18.2 51.2 25.0 51.4 19.7 56.5 16.6 2 58.7 19.9 41.2 23.2 48.7 18.1 41.0 23.9 3 50.7 21.5 36.7 21.4 39.0 21.1 33.3 22.9 4 38.0 18.2 28.3 18.1 33.7 19.5 24.7 21.3 5 29.3 20.5 21.0 15.8 28.0 17.3 18.7 20.7 6 25.3 21.3 15.3 16.1 22.7 18.5 12.0 15.7 _____________________________________________________________________ Growth Curve Parameters Initial Fear Activation 62.7 18.0 50.0 25.1 54.4 20.9 52.3 21.5 Between-Trial Fear Decline -7.7 4.6 -7.1 4.6 -6.0 3.0 -8.5 4.6 _____________ Note: Each treatment block consisted of five min. of exposure to the test chamber. Exposure Condition ____________________________________________________________________ Threat Word Neutral Word Seashore Rhythm Exposure Only (Activation) Control (Distraction) Control ______________________________________________________________________________ Measure Pre1 Pre2 Post Pre1 Pre2 Post Pre1 Pre2 Post Pre1 Pre2 Post ______________________________________________________ Peak Fear Mean 74.7 63.3 26.7 69.3 65.3 23.3 69.3 63.3 31.3 67.3 63.3 13.3 SD 15.1 17.2 18.8 16.2 11.9 26.1 17.5 16.3 26.4 17.1 16.8 24.1 HR Mean 10.2 7.6 4.4 12.9 8.7 6.6 18.8 14.1 3.3 13.9 12.2 4.2 SD 7.8 6.7 5.7 7.8 5.8 5.8 8.8 12.4 5.5 7.0 11.0 5.4 ______________________________________________________________________________ Treatment Conditions Procedures Common to All Treatment Conditions Prior to the start of each treatment trial, participants completed ratings of anticipated fear, panic likelihood, danger, and self-efficacy for the upcoming excursion. Upon exiting the chamber, participants completed ratings of fear, panic, and anxiety symptom severity. The interval between treatment trials was approximately three min. The duration of each exposure trial was recorded by the experimenter along with a running total of exposure duration. Treatment proceeded in this fashion until each participant’s total duration of exposure reached 30-min. This resulted in equivalent durations of exposure for all participants. Threat Word Condition Participants assigned to the threat word condition were instructed to attend to claustrophobic-relevant threat words (e.g., suffocate) during the entire duration of each treatment trial. Each of 15 threat words (e.g., suffocate, trapped, dark) was presented by a female voice every 10 secs. through headphones attached to a Sony Walkman. Participants were instructed to repeat aloud each word, and then form a mental image connecting them to the threat word. For example, for the word SUFFOCATE, participants were instructed to imagine running out of air in the chamber. To increase adherence to the experimental instructions, participants were informed that they would be queried about their images and tested on the words at the conclusion of the experiment. Neutral Word Condition This condition was identical to the threat word condition described above with the exception that 15 neutral words (i.e., BANANA) were repeatedly presented in place of the claustrophobic threat words. Neutral words and threat words were matched on number of syllables and word frequency. Seashore Rhythm Test Condition Participants in this experimental condition took part in a modified administration of the Seashore Rhythm Test (SRT; Halstead, 1947) during each exposure trial. This test was chosen for several reasons. First, the SRT requires continuous heavy demand on participants’ information processing, thus providing a more stringent test of the effects of distraction on fear reduction. Second, performance on the SRT is well within the capacity of normal college students, thus reducing the likelihood that participants would give up on the task prematurely due to frustration generated by poor performance. We tested several hypotheses derived from the emotional processing theory of fear reduction by manipulating claustrophobic participants' focus of attention during in vivo exposure. Sixty participants displaying marked claustrophobic fear were randomized to one of four exposure conditions. One group attended to threatening words and images during exposure and was compared to a control group that attended to neutral words and images. A third group performed a demanding cognitive load task- a modified Seashore Rhythm Test during exposure and was compared to an exposure only control group. Although the threat word manipulation resulted in greater fear activation during exposure, it was not associated with lower levels of fear following treatment. Consistent with prediction, the distraction manipulation resulted in less fear reduction at posttreatment. Treatment process analyses revealed that the negative effects of distraction on treatment outcome were primarily due to a disruption in between-trial habituation. These results and their relevance to emotional processing theory are discussed. Table 1 Group Means and Standard Deviations for the Primary Outcome Measures at Pre and Posttreatment. Table 2 Means and Standard Deviations of Subjective Peak Fear Indices and Growth Curve Parameters across the Six Treatment Blocks. Percentage of Participants Attaining Clinically Significant Improvement for the Four Exposure Conditions. Decay Lines of Maximum Subjective Fear During Treatment Participants Severely claustrophobic college students from a large southwestern university (N = 60) took part in the experiment. Participants were selected from a large subject pool (N = 2650) of introductory psychology students through a two stage screening procedure. The final sample was predominantly female (83%) and Caucasian (96%). Participants ranged in age from 18 to 51 (Mean age = 18.9; SD = 2.7). Students received partial course credit for their participation in the experiment. Measures Outcome Measures Peak Fear. Heart-Rate Reactivity. Clinical Status. (Jacobson & Truax, 1986). Treatment Process Measures Subjective Fear Indices Heart-Rate Reactivity. Mean Ratings of Maximum Subjective Fear from Behavioral Approach Tests at Pre-and Post-Treatment, and Decay Lines of Maximum Subjective Fear During Treatment for the Seashore Rhythm Test (Distraction) and Exposure-Only Control Exposure Conditions. Mean Ratings of Maximum Subjective Fear from Behavioral Approach Tests at Pre-and Post-Treatment, and Decay Lines of Maximum Subjective Fear During Treatment for the Threat Word and Neutral Word Exposure Conditions. • Our attempt to increase initial fear activation by having participants focus on threat-relevant words and images during exposure was successful as evidenced by greater initial fear activation in the threat word/image condition relative to the neutral word/image condition. Nevertheless, Those in the threat focus condition did not achieve greater overall fear reduction during treatment relative to the neutral word/image or no word/image control conditions. • Our findings do not suggest that fear activation is unimportant in fear reduction; they simple suggest that the magnitude of fear activation is unrelated to treatment outcome. • It appears that distraction exerts its detrimental effects on fear reduction through an attenuation of between-trial habituation as opposed to a dampening of fear activation.
Introduction Results Conclusions Method An Examination of the Potency of Guided Threat Reappraisal: Implications for Clinical Practice Tracy Sloan, Mark B. Powers, Jasper A.J. Smits, Victoria Beckner, & Michael J. Telch The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Participants Severely claustrophobic college students from a large southwestern university (n=69) took part in the experiment. Participants were selected from a large subject pool (n = 3000) of introductory psychology students through a two stage screening procedure. The final sample was predominantly female (72%) and Caucasian (76%), with a mean age of 22. Students received course credit for participation in the experiment. Measures Diagnostic Assessment Composite International Diagnostic Interview (CIDI.). (World Health Organization, 1997) Treatment Integrity Checks Cognitive Focus Check. Monitoring Forms. The SBU and Combo groups were asked additional questions about their use of coping strategies and the degree to which they were helpful. The GTR and Combo groups were asked additional questions aimed at enhancing disconfirmation (e.g. their ability to focus on the threats, their belief in the severity of the threat, and the likelihood of the identified threats occurring). These measures insured treatment adherence. Outcome Measures Suffocation Scale (SS). (Rachman & Taylor, 1993). Restriction Scale (RS). (Rachman & Taylor, 1993). Peak Fear. Immediately following each BAT, participants were required to rate their maximum level of fear. Clinical Significance. Based on the recommendations by Jacobson and Truax (1991). Procedure Participants were randomly assigned to one of three 30-min exposure conditions: (a) guided threat reappraisal (GTR); (b) safety behavior utilization (SBU); and (c) safety behavior utilization and guided threat reappraisal combined (SBU+GTR). Outcome assessments consisted of self-report questionnaires and subjective and behavioral responses during two consecutive behavioral approach tests. These measures were collected at pre-treatment; post-treatment; and 2-week follow-up. Treatment process indices were collected at 5-min intervals and consisted of subjective ratings of peak fear. Numerous clinical trials have demonstrated the efficacy of Cognitive Behavioral Treatment (CBT) in treating anxiety disorders (cf. Chambless & Gillis, 1993). However, a significant number of anxiety patients do not benefit (e.g., Barlow et al., 2000; Heimberg et al., 1998) and of those who do benefit, most continue to display residual symptoms and impaired work/academic impairment (Eng, Coles, Heimberg, Safren, 2001). Consequently, there is a considerable need for developing more potent psychological treatments for anxiety disorders. One fruitful approach in the investigation of fear change mechanisms is to experimentally manipulate a theoretically-relevant exposure parameter and assess the effects on fear reduction. Results of a series of experiments in our laboratory with claustrophobics have provided preliminary evidence that factors that influence the cognitive processing of disconfirming evidence have a significant effect on level of fear decline. Efforts to facilitate threat disconfirmation during exposure have met with some success. For example, providing claustrophobics with heart-rate feedback during exposure led to greater fear change than a neutral tone feedback or no feedback group. Moreover, having claustrophobics focus on their core threats during exposure and reappraise their threat between exposure trials led to greater fear change than exposure without guided threat focus and reappraisal (Kamphuis & Telch, 2000; Sloan & Telch, 2002). Alternatively, there is growing evidence that factors which interfere with the cognitive processing of threat disconfirming information may have deleterious effects on exposure-based fear reduction (cf. Craske & Rodriguez, 1998). For example, providing claustrophobics with cognitive load tasks during exposure lessens the overall level of fear decline a deleterious effect on fear reduction (Kamphuis & Telch, 2001; Telch et al., 2003). For example, subjects who were required to engage in a demanding dual process cognitive load arithmetic task during treatment displayed less fear reduction than a group that received the same duration of exposure without the cognitive load task (Kamphuis & Telch, 2001). These findings are consistent with the conclusions of Rodriguez and Craske (1994) in their review of the effects of distraction on exposure-based fear reduction. Taken together, research supports the idea that safety behavior utilization impedes fear reduction, whereas guided threat reappraisal techniques facilitate fear reduction. The question arises whether practitioners would benefit from identifying safety behaviors and fading their use even when applying GTR. Therefore, the present study further examined the potency of detrimental effects of safety behavior utilization, by testing whether safety behaviors continue to exert a negative effect even when combined with GTR. Peak Fear during the BAT at Pre-, Post-, and Follow-up. Percent Achieving Clinically significant Change at Post- and Follow-up. • Consistent with predictions: • Our findings are in accord with those from the Oxford Group (Salkovskis et al, 1999, Wells et al, 1995) suggesting that making safety aids available to patients may actually undermine the efficacy of exposure-based treatments. • Clinicians may benefit if they identify safety strategies used by the patient during exposure to feared activities, and to encourage and assist the patient in discarding these safety behaviors.
Exposure Condition ______________________________________________________________ Threat Word Neutral Word Seashore Rhythm Exposure Only (Activation) Control (Distraction) Control ______________________________________________________________________________ Measure M SD M SD M SD M SD ______________________________________________________________________________ Treatment Block 1 59.1 18.2 51.2 25.0 51.4 19.7 56.5 16.6 2 58.7 19.9 41.2 23.2 48.7 18.1 41.0 23.9 3 50.7 21.5 36.7 21.4 39.0 21.1 33.3 22.9 4 38.0 18.2 28.3 18.1 33.7 19.5 24.7 21.3 5 29.3 20.5 21.0 15.8 28.0 17.3 18.7 20.7 6 25.3 21.3 15.3 16.1 22.7 18.5 12.0 15.7 _____________________________________________________________________ Growth Curve Parameters Initial Fear Activation 62.7 18.0 50.0 25.1 54.4 20.9 52.3 21.5 Between-Trial Fear Decline -7.7 4.6 -7.1 4.6 -6.0 3.0 -8.5 4.6 _____________ Note: Each treatment block consisted of five min. of exposure to the test chamber. Introduction Results Conclusions Method Salivary Cortisol Perturbations in Claustrophobic Patients in Response to Phobic Stimuli and Normalization Following Exposure-Based Treatment: A Work in Progress Mark B. Powers, M.A., Victoria Beckner, M.A., Jasper A.J. Smits, M.A., & Michael J. Telch, Ph.D. The University of Texas at AustinLaboratory for the Study of Anxiety Disorders Data suggest that compared to healthy controls, social phobic, PTSD, and panic disorder patients exhibit an abnormal cortisol response to their feared stimuli. Further, this deviation appears specific to phobic stimuli with few baseline differences or abnormalities during other stressors (i.e. exercise, mental arithmetic, cold pressor, etc.). However, it is not known if this abnormal cortisol perturbation is apparent in specific phobias such as claustrophobia. More importantly, it is unclear if this response normalizes following successful treatment. Preliminary results suggest that there is an exaggerated cortisol response in the claustrophobic group. Moreover, cortisol levels among claustrophobic participants appear to normalize following treatment. Participants Participants were selected from a large pool of approximately 5000 introductory psychology students from the University of Texas at Austin through a two-stage screening procedure. They were given course credit in return for their participation. The final sample (N=72) consisted primarily of women (86%), ranging in age from 18 to 49 (M = 21.06; SD = 5.07). Most participants (75%) met full DSM-IV (American Psychiatric Association, 1994) criteria for claustrophobia, while 25% met all DSM-IV criteria with the exception of Criterion E (i.e., the person must experiences significant interference in social, academic or work functioning or experiences marked distress about having the phobia). The ethnic breakdown of the sample was 74 % Caucasians, 13% Mexican-American, 7% African-American, 5% Asian-American, and 1% Indian-American. Design Participants were randomly assigned to one of three conditions: (1) exposure only, (2) placebo, or (3) wait-list control. A behavioral assessment (BAT) was conducted before and after treatment with salivary cortisol collection prior to and following the BAT. Cortisol assays obtained from this sample were contrasted to a second group of healthy controls who underwent the same protocol, but without exposure treatment. • Cortisol perturbations are present in Claustrophobia • These differences appear to normalize with exposure-based treatment • It remains unclear if these observations are indicative of a predisposition or simply disease sequale.