Download
1 / 45
460 likes | 1.2k Vues
Introduction : Vascular anomalies. Vascular lesions in the head and neck region can result in significant cosmetic problems for the patient, and some may lead to even serious life threatening hemorrhage.. Vascular anomalies. In the past, there has been confusion regarding the proper nomenclature for vascular lesions.In 1982, Mulliken and Glowacki

E N D
1. Vascular Anomalies - A Review
Division of Oral and Maxillofacial Surgery
College of Dentistry
King Saud University.
3. Vascular anomalies
In the past, there has been confusion regarding the proper nomenclature for vascular lesions.
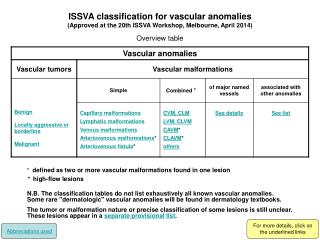
In 1982, Mulliken and Glowacki �biologically classified� the vascular anomalies of the maxillofacial region based on their clinical behavior and endothelial cell characteristics into two groups: hemangiomas and vascular malformations.
4. Hemangiomas
Hemangiomas, are the most common tumors of the head and neck in infancy and childhood, comprising approximately 7% of all benign soft tissue tumors .
5. Development : Hemangiomas The hemangioma is a true vascular tumor that results from a overgrowth of normal vascular tissue .
It exhibits relatively rapid early growth until approximately 6 to 8 months of age (proliferative phase), followed by regression by 5 to 9 years of age (involutory phase).
It grows by �endothelial proliferation�. During the rapid
growth phase, an increased number of mast cells is seen
within the endothelial wall.
6. Development : Hemangiomas The majority of the hemangiomas in infants are noted by the parent within the first month of life.
Hemangiomas are initially noticed as an erythematous, macular patch, which progresses through a rapid proliferative phase whereby it changes its color and grows faster than the commensurate growth of the child.
By the time the patient is 12 months of age most hemangiomas have shown signs of involution. The process of involution is normally slow and will not be completed until the age of 5 to 9 years.
7. Clinical presentation : Hemangiomas Hemangiomas are found in the superficial tissue, the deep tissue, or both and may affect organ systems such as the liver, lung, spleen, and gastrointestinal tract.
Most superficial hemangiomas can be diagnosed by clinical examination and a detailed and accurate history.
8. Clinical presentation : Hemangiomas
Deep hemangiomas involve muscle or visceral organs and, are more difficult to diagnose. Therefore, further diagnostic studies are required.
Intra-osseous hemangiomas are extremely rare. However the soft tissue lesion may deform the underlying skeleton.
The predilection for females is approximately a 3 :1 ratio.
9. Clinical presentation : Hemangiomas On examination, the superficial hemangioma usually consists of a raised, reddish to purple tumor with a distinct margin.
In contrast, deep subcutaneous hemangiomas often have a deep bluish hue with normal overlying skin, making diagnosis more difficult.
Both the lesions are firm to palpation and do not pulsate or exhibit any thrills or bruits.
10. Investigations : Hemangiomas Computed tomography (C. T .Scan) and Magnetic resonance imaging ( M. R. I) imaging techniques are used as diagnostic aids to document the extent of the deep hemangiomas.
11. Investigations : Hemangiomas
Arteriography is rarely indicated for the diagnosis of a hemangiomas.
12. Management : Hemangiomas Observation and parental support are the initial approaches in the management of maxillofacial hemangiomas.
If functional compromise such as visual change, airway or masticatory compromise, bleeding, ulceration, or infection occurs intervention is necessary.
13. Management : Hemangiomas This may initially involve cortico-steroids for rapidly proliferating lesions or therapy with interferon alfa-2a.
Surgery is generally reserved for small lesions and as a secondary procedure after initial therapy and involution.
Treatment modalities include routine excision, injection of sclerosing agents, cryotherapy, and ablation using an argon laser.
14. Vascular Malformations
Vascular malformations are present at birth and unlike hemangiomas, do not go through a a �rapid proliferative phase� and they do not �involute�.
They grow commensurately with the patient.
15. Vascular Malformations - Types
Vascular malformations may be capillary, venous, arterial, or combinations of these.
Approximately 31% of these malformations are found in the head and neck region.
16. Vascular Malformations Vascular Malformations are divided into two categories: Low-flow and High-flow lesions.
Capillary, venous, and lymphatic malformations exhibit �low flow lesions�.
Arterial and arterio-venous malformations exhibit �high flow� and are capable of severe hemorrhage with significant morbidity.
17. Development : Vascular Malformations
Vascular malformations are thought to �result when there is interruption at a particular stage of development of a vessel�.
The type of vascular malformation that results depends on the stage at which normal morphogenesis is interrupted.
18. Development : Vascular Malformations
Thus, vascular malformations are sub-classified by tissue type into capillary, venous, arterial, lymphatic, and combinations thereof, with the type of malformation that develops depending on the type of tissue affected during abnormal development.
19. Development : Vascular Malformations
Trauma, infection, and hormonal fluctuation (pregnancy or puberty) may stimulate increased growth of the vascular malformation.
The mechanism of growth is not increased endothelial proliferation - which is within a normal range in these lesions, as is the number of mast cells � �but alteration in the flow dynamics within and around the lesion�.
20. Development : Vascular Malformations
This results in recruitment of �collateral vessels� and dilatation of involved vessels.
Unlike the hemangioma, the vascular malformation exhibits a steady increase in growth, without signs of involution.
21. Clinical presentation : Vascular Malformations
In many cases, the diagnosis of a vascular malformation can be made from the patient�s history.
Although present at birth, these lesions are often not identified immediately, but only later on when the lesion enlarges enough to be clinically identifiable. This is particularly true for intra-bony lesions.
22. Venous Malformations - Low-flow lesions
Venous malformations are bluish, soft and easily compressible, and auscultation reveals no bruits.
These malformations can vary from superficial, localized, mucosal spongy ectasis to complex invasive lesions that permeate tissue planes and alter the regional anatomy.
23. Venous Malformations Any maneuver that increases venous pressure (e.g.Valsalva maneuver or supine positioning) can temporarily enlarge a venous malformation.
The clinical absence of �pulsations or a thrill� generally indicates a low flow Venous vascular malformation.
Phleboliths that may be noted on radiographic examination are found only in low flow lesions.
24. Venous Malformations - Phleboliths
25. Capillary Malformations - Low-flow lesions
Capillary malformations may be smooth initially but become more � pebble � like� as the patient grows.
Intra-orally, these lesions are often comprised of lymphatic tissues and therefore take on an irregular, pebbly surface; sometimes called as �salmon eggs�.
26. Capillary Malformations - Low-flow lesions Port-wine stains, telangiectasias and capillary malformations may appear pink in infancy and darken to a deep purple in childhood.
27. Capillary Malformations: Familial Telengectiasis
28. Lymphatic Malformations - Low- flow lesions
Lymphatic malformations are normally colorless; however, combined lesions take on the hue of the additional vessel type.
�Lymphatic-venous malformations� may appear deep purple while �capillary-lymphatic malformations� can be pink to purple.
These malformations can become invasive by dissecting along tissue planes and can cause bony hypertrophy, distortion or both. As these are lymphatic tissues, infections may result in rapid enlargement of these lesions.
29. Lymphatic Malformations � �Low- flow lesions�
30. Arterial / Arteriovenous Malformations - �High-flow lesions� Arterial or AV Malformations are high flow lesions, which consist of a large high-flow vessel leading into a multitude of smaller lower-flow lesions.
It is the lower-flow vessels which induce the development of the feeder vessels.
Thus the resulting collateral circulation makes these malformations very difficult to manage.
31. Arterial / Arteriovenous Malformations
Clinically these lesions appear stained, warm and tender to palpation. There may be swelling or asymmetry.
A bruit may be detected.
32. Arterial / Arteriovenous Malformations Often a patient presents with severe bleeding as the first sign that a high flow-lesion is present. They may also complain of recurrent gingival bleeding and loose or depressible teeth.
33. Investigations : Vascular Malformations
Many vascular malformations demonstrate few radiographic signs until well into adolescence and a significant percentage will never show any bony changes.
If the lesion involves bone, then a �soap bubble� or a �honeycomb appearance� is the usual radiographic finding.
34. Investigations : Vascular Malformations
Magnetic resonance images (MRI) may differentiate low-flow from high flow lesions. The presence of fatty deposits, venous lakes, phleboliths in the MRI are all indicative of low- flow lesions.
CT scans document a lesion�s extension into the surrounding soft tissue.
Doppler imaging can also distinguish high flow lesion from low flow lesions.
35. Investigations : Vascular Malformations Arteriography cannot only delineate the size of the lesion, but can also assess the rate of flow through the lesion.
Moreover, super-selective embolization of the selective feeding vessels to the high flow vascular lesion can be achieved simultaneously while performing the arteriography procedure.
This procedure is usually done before surgery, in order to prevent the risk of serious hemorrhage during surgery.
36. Management : Capillary Malformation
In the head and neck area, the �argon laser� has proven to be very effective in altering unsightly superficial blemishes that are caused by capillary malformations, port-wine stains and other telangiectasias.
37. Management : Capillary Malformation
It is important to remember that port-wine stains may occur in association with lymphatic, venous or arterial malformations. Therefore, it is important that management of these cases be based upon the characteristics of any deeper malformation.
38. Management : Lymphatic Malformation Lymphatic malformations can prove to be more difficult to treat because of the poor demarcation and the infiltrative nature of the lymphatic vessels.
Therefore for the lymphatic malformations several non-surgical modalities like steroid therapy, radiation therapy and sclerotheraphy are available.
Bleomycin sclero-therapy, O.K 432 sclerotheraphy are found to have promising results in the treatment of lymphatic malformations prior to and possibly precluding surgical intervention.
39. Management : Venous Malformation Some of the Low-flow Venous malformations lesions may cause bleeding during surgery, and therefore it is important to determine the lesions size and flow dynamics with the help of arteriography before surgery.
The treatment of a true low flow venous malformation is based on the size and location of the lesion.
40. Management : Venous Malformation
Sclerosant theraphy alone has been shown successful for smaller malformations. Direct injections of sodium morrhuate, boiling water, alcohol, and Ethibloc have proven to be effective in fibrosing these smaller lesions.
Larger, invasive malformations have been treated with a combination of sclerosant and surgical therapies.
41. Management : Venous Malformation
Kane et al. have recently demonstrated significant patient satisfaction with sclero-therapy with tetradecyl sulfate (Sotrdecol) combined with conservative ablation.
It is important to know that in most cases sclerosant therapy is purely an adjunct to proper surgical ablation.
42. Management : Arterial or A-V Malformation High flow lesions can have turbulent blood flow, introducing the risk of consumption coagulopathies. Therefore proper pre-operative hematological studies have to be carried out.
Pre-ablation selective arterial embolization has improved the surgical success rates for arterial and A-V Malformations, especially the intra-osseous ones.
43. Management : Arterial or AV Malformation The goal of embolization is to decrease flow in the malformation while avoiding disruption of flow through proximal feeders.
Any surgical intervention should follow within 24 to 48 hours of embolization, and never later than 10 days. It is believed that collateral flow to the malformation develops soon after embolization and that delaying surgery increases the possibility of intra-operative bleeding and postoperative recurrence.
The goal of surgery should be total excision of the malformation.
45.
THANK YOU