Download
1 / 59
620 likes | 729 Vues
ENERGY BALANCE. S. Zahedi Endocrine Research Center Research Institute for Endocrine Sciences Shaheed Beheshti University of Medical Sciences 2 nd obesity Congress 29-30- Oct. 2009 Tehran-Iran.

E N D
ENERGY BALANCE S. Zahedi Endocrine Research Center Research Institute for Endocrine Sciences ShaheedBeheshti University of Medical Sciences 2nd obesity Congress 29-30- Oct. 2009 Tehran-Iran
One of the myths of the modern world is that health is largely determined by individual choice. Barry R. Bloom (2000) Each individual has his or her predetermined energy ration= if some body uses slowly, lasts longer
Genes Susceptibility genes (many genes, each with small effect) Monogenic syndromes OBESITY ENERGY BALANCE Physical activity Food intake Environment/Lifestyle
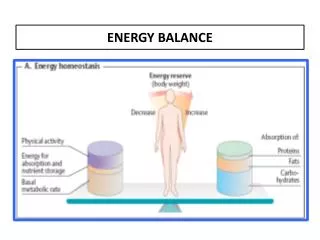
Energy Balance Basal metabolism: energy expenditure of a subject relaxed and at rest, at thermoneutrality, 8–12 hours after last food ingestion. Adaptive thermogenesis: energy dissipated as heat in response to environmental changes.
Nervous Control systems in the body Hormonal
Feeding Experiments • Forced feeding • Measure size of food • Introduce food for some time more than what the animal consumes ( force feeding) • Will lead to weight gain • If you remove force feeding, will lead to reduced food consumption for some time • Will return to previous value • Restricted food ration • Measure size of food • Introduce restricted food size for some time (less than what the animal consume • Will lead to weight loss • If you remove restricted feeding, will lead to increased food consumption for some time • With return to previous value
Brain Lesioning Studies • Profound obesity from destruction of hypothalamic: • Paraventricular nucleus (PVN) • Ventromedial nucleus (VMN) • Dorsomedial nucleus (DMN) • Anorexia/weight loss from destruction of: • Lateral hypothalamic area (LHA)
Brain Centers in Energy Homeostasis NPY AgRP ARC: arcuate nucleus, PVN: paraventricular nucleus, PFA: perfornical area, FX: fornix, LHA: lateral hypothalamic area, VMN: ventromedial nucleus, DMN: dorsomedial nucleus, AM: amygdala, CC: corpus callosum, OC: optic chiasm, SE: septum, TH: thalamus, 3V: third ventricle
Phases of food in GI tract • Cephalic Phase • CNS is involved • Vagus nerve • Gastric Phase • Presence of the food in the stomach ( Involvement of ENS • Vagus nerve is involved ( Vago-Vagal Reflex) • Enteric Phase • ENS is involved • Vagus nerves is involved • GI Hormones
Food intake control stages • Very short term • Short term • Long term
Food intake control stages • Very short term • Sham satiety • Pure nervous • Ends food consumption during each meal • Eosophagus • Mechanoreceptors • Counts the bolus • Convey the signals to CNS • Stomach • Mechanoreceptors • Counts the bolus • Stimulated by stretch • Convey the signals via vagus nerve • Vagotomy remove this signal • Short term • Through satiety • Glucose ( Glucostatic) • AA ( aminostatic) • Temp.( thermostatic) • Plasma osmolarity ( Osmostatic) • GI hormones • Long term • Contents of Adipose Tissue • Signals from fat cells to CNS • Controls energy content of the body (body weight)
SET POINT HYPOTHESIS • Blood-borne factor(s) mediate(s) control of body weight at a defined level (the "set point") by interacting with the hypothalamus • Factors regulate: • food intake (appetite) • energy expenditure (level of activity and body temperature) • Several discrete genetic loci and their protein products identified • Efficiency or defect in one of these may disrupt normal weight control leading to dramatic weight gain and associated syndromes (e.g., NIDDM) • 80% of NIDDM cases are associated with obesity • Model of food intake: lipostat (adipostat) concept = signals proportional to the size of fat stores integrate with other regulators of food intake • Depletion of energy stored in adipose tissue increases food consumption => larger meal sizes • Food intake is regulated within a lipostatic system for energy homeostasis
Appetite is suppressed CNS MSH from POMC neurons Periphery Metabolic activity increases to burn fat Leptin + Hypothalamus arcuate nucleus JAK-STAT3 Leptin receptor Adipose Adipose stores are HIGH
Appetite is enhanced JAK-STAT3 CNS Periphery Metabolic activity decreases limiting fat burning Leptin + Leptin receptor Hypothalamus AGRP from hunger neurons Block MSH binding MSH Adipose Adipose stores are low
Control of Feeding Behavior and Satiety Figure 24.23
Conclusion • Physiological control of food intake and energy intake are very efficient, If we leave the m alone, they will work perfectly. • Any deviation in their activity whatever is the reason will obviously change the balance in away that we do not want • Some of these deviations may have pathological nature, but some of them are because of our behavior, it is better to leave them to themselves.!!!!!!!!!!!!!!!
Profusion of Peripheral Signals DVC: Dorsal Vagal Complex
Dopamine and Outputs to Striatum (motor activity) (motivation/reward) SNPC: substantia nigra pars compacta VTA: ventral tegmental area Opioids and amphetamines remove a GABAnergic block on dopamine production. These drugs suppress appetite, and were initially used to treat obesity. In humans, BMI is anti-correlated with #D2 receptors in the striatum.
Bias Toward Weight Gain Arc destruction causes weight gain. Response to weight loss bidirectional; weight gain unidirectional. DMc4r=> weight gain whereas Dnpy=>no weight loss. AgRP/Npy neurons are more sensitive to adiposity signals than Pomc/Cart neurons. HOWEVER: Anabolic pathways are required for intact responses to negative energy balance (IDDM causes negative energy balance in Npy-/- mice). Anabolic pathways are required for response to decreased leptin (Npy-/- over ob/ob mice show reduced hyperphagia).
Currently Approved Therapies Orlistat (interferes with fatty acid hydrolysis); => moderate clinical effects; side effects include gas/diaharrea. Sibutramine (central norepinephrine/serotonin RI); => moderate clinical effects; side effects include tachycardia and hypertension. Roux-en-Y gastric bypass (absorption and hormonal). 4. Rimonabant (Acomplia; CR1 endocannabinoid antagonsist).
Adipokines • Adipokine is a term applied to biologically active substances found in the adipocytes of white fat (adipose) tissue. • Adipokines may be synthesized at other sites and participate in functions unrelated to those within adipose tissue. • Many exert proinflammatory effects and may be causally involved in obesity and diabetes. • These adipokines include • leptin, • tumor necrosis factor alpha (TNFα), • interleukin (IL)-6, • plasminogen activator inhibitor-1 (PAI-1), • angiotensinogen, • and resistin. • A few others, particularly • adiponectin and transforming growth • factor beta-1 (TGF-β1), are anti-inflammatory and may exert protective functions against metabolic disturbance.
Leptin receptors in the CNS • High levels of leptin receptor mRNA and protein are expressed in both rodent and human • In Hypothalamus: • (ventromedial hypothalamus, • arcuate nucleus • and dorsomedial hypothalamus) that are involved in regulating energy homeostasis are highly enriched with leptin receptors.
Leptin receptors in the CNS • Leptin receptor mRNA and immunoreactivity are also highly expressed in many extra-hypothalamic brain regions including: • hippocampus, • brain stem, • cerebellum, • amygdala and • substantia nigra
Leptin In CNS • Leptin is thought to enter the brain via two distinct mechanisms. • A saturable transport system is thought to enable leptin to cross the blood brain barrier via receptor-mediated transcytosis • Short leptin receptor isoforms, which are capable of binding and internalizing leptin, have been detected on brain microvessels
In addition, • It appears that leptin is made and released locally in the CNS. • mRNA and immunoreactivity are widely expressed throughout the brain • So is it a neurotransmitter??? (Morash et al, 1999;Ur et al, 2002).
What is a neurotransmitter??? • Can be synthesized in the nervous system • Released in the synaptic cleft • Act through post synaptic membrane • Modify postsynaptic membrane potential
Previous studies have demonstrated that leptin inhibits: • Peripheral insulin-secreting cells • Glucose-responsive hypothalamic neurons and • Nucleus tractussolitarius neurons • Via activation of ATP-sensitive potassium (KATP) channels. • Similarly leptin inhibits rat hippocampal neurons by • Increasing a K+ conductance • It seems Ca2+-activated K+ channels are involved.
Leptin alter synaptic function • Leptin alter the strength of excitatory synaptic transmission under conditions of enhanced Excitability . • In certain conditions leptin cause hippocampal long-term depression (LTD) • In contrasts leptin under physiological conditions (1 mM Mg2+), it promotes the induction of hippocampal long term potentiation (LTP).
Leptin, learning and memory • Recent studies have implicated leptin in associative learning and memory : • leptin-insensitive (db/db mice and fa/fa rats) rodents display impairments in hippocampal long-term potentiation (LTP) and long-term depression (LTD), as well as deficits in spatial memory tasks . • Direct administration of leptin into the hippocampus enhances LTP in vivo. • At the cellular level, leptin converts hippocampal short lasting potentiation (STP) into LTP • Leptin also contributes to synaptic plasticity changes in the hypothalamus as the efficacy of inhibitory and excitatory synaptic transmission is altered in leptin-deficient ob/ob mice
Leptin and Morphological changes • Leptin increases the number of dendritic filopodia in hippocampal neurons • Leptin induces actin re-organisation in hippocampal neurons • Leptin enhances actin-based motility of filopodial extensions • Leptin promotes formation of functional hippocampal synapses
Blood Brain Barrier • Large interface (100-150 Cm2/kg) between circulation and the brain • Monolayer of endothelial cells • Few fenestrations • Few Pinocytic vesicles • Few transendothelial channels • Are joined by tight junctions • Continuous basement membrane • Astrocyticendfeet • Pericytes • Controls penetration of AA, Peptides, proteins,…
Blood-brain barrier (BBB) • The BBB constitutes a large interface between the circulation and the central nervous system (CNS), consisting of: • brain and • spinal cord. • Its primary component is a monolayer of endothelialcellsforming the outer wall of capillaries and venules. • These microvascular endothelial cells have few fenestrations, pinocytic vesicles, or transendothelial channels, and are joined by tight junctions. • A continuous basement membrane, astrocyticendfeet, and pericytes reinforce barrier function from the basolateral side facing the extracellular matrix. • The surface area of the BBB is 100 to 150 cm2/g,. • This immense neurovascular interface controls the penetration of amino acids, peptides, polypeptides, and proteins as well as many other molecules .