Download
1 / 24
270 likes | 649 Vues
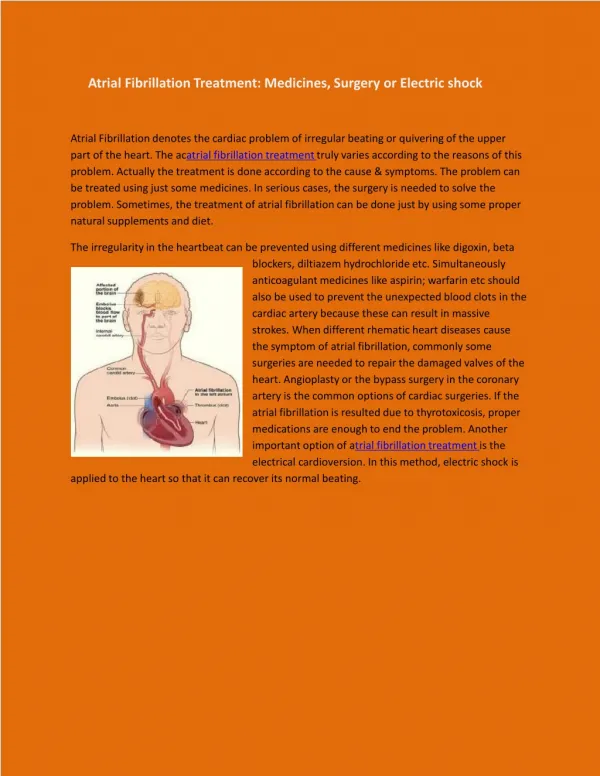
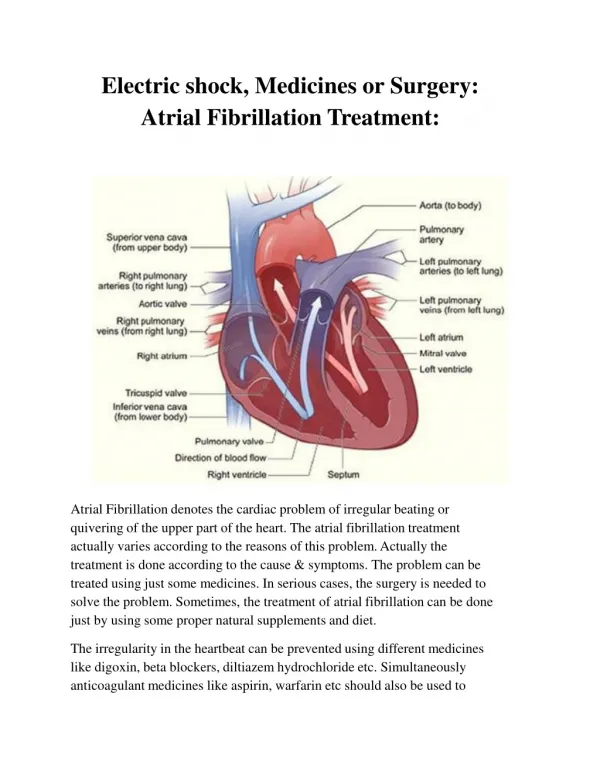
SURGICAL TREATMENT OF ATRIAL FIBRILLATION. 1/ Incidence of AF: 5% of the population > 60 years, - 600 000 candidates for AF surgery in USA 2/ Etiologies: among patients applying for a life insurance: 40% lone AF, 60% with cardiopathy

E N D
SURGICAL TREATMENT OF ATRIAL FIBRILLATION 1/ Incidence of AF: 5% of the population > 60 years, - 600 000 candidates for AF surgery in USA 2/ Etiologies: among patients applying for a life insurance: 40% lone AF, 60% with cardiopathy 3/ Restoration of sinus rhythm after valve repair depends upon the duration of AF (> 1year) and left atrium dimensions (>60mm) 4/ The presence of preoperative AF does not influence the operative risk Specific surgical procedures aiming at treating atrial fibrillation must add minimal morbidity Chua JTCS 1993 & Obadia JTCS 1997
ATRIAL EXCLUSION LINES which tracing? 1/ Original Cox-Maze III procedure 2/ Hemicox: left maze procedure 3/ Exclusion of the pulmonary veins (+ left appendage exclusion)
CLASSICAL COX-MAZE III left appendage right appendage sup. veina cava septal incision pulmonary veins tricuspid mitral inf. veina cava
LEFT COX-MAZE PROCEDURE left appendage pulmonary veins mitral
EXCLUSION OF THE PULMONARY VEINS left appendage pulmonary veins
COX-MAZE PROCEDUREassociated to mitral valve surgery N = 40 Indications: Chronic AF > 6 months 35 Intermittent AF (left maze) 5 AGE: 15-71 YRS (49+16 YRS) ETIOLOGIES OF MITRAL VALVE DISEASE: degenerative 20 rheumatic 17 others 3
MITRAL VALVE PROCEDURE associated to the Cox-maze MAZE DURATION complete: 52 min left: 23 min
mortality: 1 (2,5%) (septic shock) reoperation for bleeding: 3 coronary bypass for circumflex stenosis 1 pace maker (complete maze) 1 fluid retention (complete maze) 4 lower limbs edema : 4 pericardial effusion: 2 pleural effusion: 2 RESULTScomplete maze = left maze
POSTOPERATIVE EKGcomplete maze = left maze n = 39 immediate 1 month AT 1 MONTH, FREEDOM FROM AF: 75%
18 pts with complete maze LATE EKG 1 month 1 year AT ONE YEAR: FREEDOM FROM AF: 69%
POSTOPERATIVE TREATMENT anticoagulants antiarhythmics Transient stroke at 10 mths, sinus with AC : 1
DOPPLER following COX-MAZE PROCEDURE evidence for atrial transport e e a a tricuspid flow mitral flow
ATRIAL WALL in chronic atrial fibrillation fat transformation muscular hypertrophy C. Guiraudon in La fibrillation auriculaire JY Le Heuzey 1997 p51
COX-MAZE PROCEDURE INDICATIONS AF indication N intermit. / chronic lone AF other Cox World Heart Foundation Schaff 221 20% 80% 25% 75% Mayo Clinic Mc Carthy 100 22% 78% 23% 77% Cleveland Clinic Izumoto 104 0% 100% 0% 100% Iwate, Japon 308 58% 42% 56% 44%
COX-MAZE OPERATION RESULTS CPB mortality fluid ret. pace maker Cox - 2,9% 6% 15% World Heart Foundation Schaff 122 mn 1,4% - 3,2% Mayo Clinic Mc Carthy 120 mn 1% yes 6% Cleveland Clinic Izumoto 177 mn 2% - 6% Iwate, Japon
COX-MAZE OPERATION RESULTS free from AF free from AF postop. intermittent AF late 99% 38% 99% World Heart Foundation Schaff 90% 38% 70% 3 yrs Mayo Clinic Mc Carthy - 33% 90% 3yrs Cleveland Clinic Izumoto 72% - 65% 5yrs Iwate, Japon
COX-MAZE OPERATION RECENT ADVANCES 1/ Results of patients with rheumatic vs degenerative MV disease are identical Lee, Annals 2003:75:57-61 2/Right sided maze does not arrythmogenic substrate of lone AF and may not be necessary Jessurun, Europace 2003;5:39-46 3/ The maze operation does not influence atrial volumes in patients with lone AF / mitral surgery reduces LA volume Jessurun, Annals 2003;75:51-6 4/ The left maze can be performed through a minimally invasive approach Akpinar, Eur J Card Surg 2003;24:223-30
ENERGY SOURCES which ablation technique? 1/ Surgical cut and sew = GOLD STANDARD 2/ Radiofrequency 3/ Cryogenic injury TRANSMURALITY ? 4/ Microvawe
RADIOFREQUENCY ABLATION technical approach endocardial epicardial
RADIOFREQUENCY ABLATION epicardial & endocardial probes histology showing transmural lesion
N AF Intermit. chronic Surgery mitral aortic/CABG Le Tourneau Eur Soc Card 2003 69 19% 50% 100% - Sie Eur Soc Card 2003 200 0% 100% 81% 19% Benussi Eur JCS 2003:17;524 132 8% 92% 98% 2% RADIOFREQUENCY PROCEDURE INDICATIONS
6 months AF free Intermit. Chronic 3 years AF free Le Tourneau Eur Soc Card 2003 67% 21% 12% Sie Eur Soc Card 2003 73% Benussi Eur JCS 2003:17;524 79% - - 77% RADIOFREQUENCY PROCEDURE RESULTS
RADIOFREQUENCY ABLATION RECENT CONCEPTS 1/ No transmurality when atrial wall thickness > 4 mm 2/The epicardial is less efficient than the endocardial approach (epicardial fat + circulating blood) Thomas, Annals 2003:75:543-8 3/ Atrioesophageal fistula is a potential complication: cachectic patient, LA ectasia, TEE probe Mohr, J Thorac CVS 2002;123:919-27 4/ Circumflex coronary stenosis is a potential complication Fayad, Annals 2003;76:1291-3 5/ Age at surgery and postop arrhytmias are predictive factors of a negative outcome Benussi, Eur J Card Surg 2003;17:524-9
CONCLUSIONS 1/ The Cox-Maze operation is very efficient in restoring normal sinus rhythm in chronic or intermittentAF and remains the gold standard 2/ The left maze seems to be as efficient as the complete maze in pts with mitral valve disease 3/ Radiofrequency ablation could be an important adjunct in pts with lone/non-mitral related AF 4/ Antiarrhythmics are often necessary to maintain a good long term results 5/ The TE risk is decreased but not eliminated