Download
1 / 28
300 likes | 856 Vues
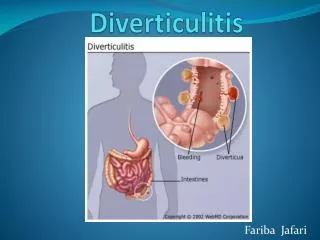
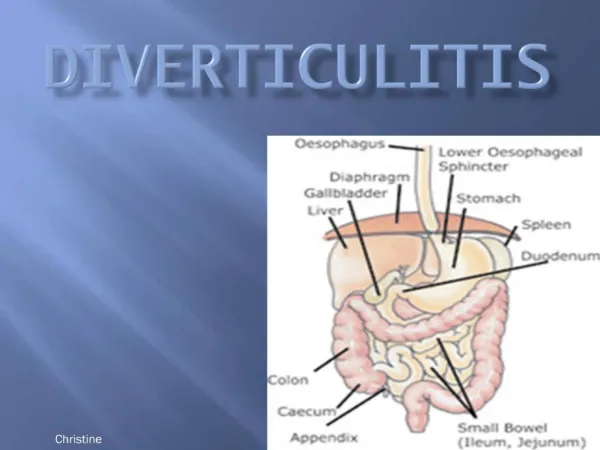
Diagnosis of diverticulosis and diverticulitis. Tryggvi Björn Stefánsson Dept of Surgery Landspitali University Hospital. Diverticulosis. Barium Enema. Barium Enema. Diverticulitis. Clinical classification Hinchey classification Ambrosetti classification.

E N D
Diagnosis of diverticulosis and diverticulitis Tryggvi Björn Stefánsson Dept of Surgery Landspitali University Hospital
Diverticulosis • Barium Enema.
Diverticulitis • Clinical classification • Hinchey classification • Ambrosetti classification
Clinical classification(European association for endoscopic surgeons) I. Symptomatic uncomplicated disease. Fever, crampy abdominal pain, CT evidence of phlegmonous diverticulitis. II. Recurrent symptomatic disease. Recurrence of above. III. Complicated disease. (hemorrhage, abscess, perforation, purulent and fecal peritonitis, stricture, fistula, small-bowel obstruction due to postinflammatory adhesions)
Hinchey classification • Stage 1 • Pericolic or mesenteric abscesses. • Stage 2 • Walled off pelvic abscess. • Stage 3 • Generalised purulent peritonitis. • Stage 4 • Generalised fecal peritonitis
Ambrosetti’s CT Staging of Diverticulitis. • Mild Diverticulitis Localized sigmoid wall thickening (less than 5 mm) Inflammation of pericolic fat. • Severe Diverticulitis Abscess Extraluminal air Extraluminal contrast
Complicated diverticulitis • Abscess • Purulent peritonitis • Faecal peritonitis • Colovaginal fistula • Colovesical fistula • Colocutan fistula • Stricture • Hemorrage
Differential diagnosis • Appendicitis. • Inflammatory bowel disease(Crohn’s disease). • Pelvic inflammatory disease. • Tubal pregnancy. • Tuboovarian abscess. • Cystitis. • Advanced colonic cancer. • Infectious colitis. • Colorectal cancer.
Diagnostic tools • Clinical symptoms. • Lab tests. • Barium enema. • Ultrasound. • MRI. • CT. • Laparoscopy.
Clinical symptoms The AVOD study: Chabok A et al, British Journal of Surgery 2012
Computed Tomography • Diverticulas • Thickening of the bowel wall >3 mm-5mm. • Cloudy fat in the mesentery
CT • Sensitivity 93%-98% • Specificity 75%-100% • Stefánsson T, Acta Radiol. 1997 Mar;38(2):313-9. • Doringer E. Crit Rev Diagn Imaging 1992; 33: 421–35 • Hulnick DH et al, Radiology,1984; 152: 491–95. • Cho KC et al, Radiology 1990; 176: 111–15. • Ambrosetti P et al Dis Colon Rectum 2000; 43: 1363–67.
Barium Enema • Diverticulas • Edema • Intramural sinus tract. • Extravasated contrast material outlining an abscess cavity. • Fistula.
Barium Enema • Sensitivity 0.82 (95% CI: 0.71-0.90) • Specificity 0.81 (95% CI: 0.67-0.91) Stefánsson T, Acta Radiol. 1997 Mar;38(2):313-9.
Ultrasound • Inflamed segment. • Hypoechogenic thickening of the bowel wall (Hypertrophy of muscularis propria) • Hyperechogenic halo (Pericolitis, inflammatory fat) • Diverticulum with hyperechogenic halo. • Luminal narrowing. • Hypoperistalsis. • Pericolic abscess.
Ultrasound • Operator dependent • Sensitivity 98.6% • Specificity 96.5% • Schwerk WB, Zeitschrift für Gastroenerologi 1993
Ultrasound • Inflammatory target sign in the left lower quadrant, • Hyperechogenic halo and diverticula. • Highly suggestive of ACD in a symptomatic patient. • Surgeons in training showed 84% sensitivity for US diagnosis . Comparable to the results of specialists. • A. Zielke, Surgical Endoscopy 1997.
US vs CT • Sensitivity • US : 92% (95% CI:80%-97%) • CT 94% (95%CI: 87%-97%) (p=0.65). • Specificity • US 90% (95%CI: 82%-95%) • CT 99% (95%CI: 90%-100%) (p=0.07). • Alternative diseases sensitivity ranged • between 33% and 78% for US and • between 50% and 100% for CT • Wytze Laméris, Eur Radiol (2008) (metatanalysis)
Magnetic Resonance Imaging • Uncomplicated diverticulitis • Diverticula • Bowel wall thickening ( more than 3-5 mm) • Pericolonic fat stranding • Complicated diverticulitis • Diverticula • Bowel wall thickening more than 5 mm • Perforation, Abscess • fistula
Laparoscopy • Acute abdomen • Acute abdomen due to diverticulitis Differentiate between purulent peritonitis and faecal peritonitis. • Recurrent diverticulitis or cronic diverticulitis to decide if the patient must be operated or not.
Summary. • Lower abd pain, tenderness and raised CRP. • US ? If in doubt CT or MRI. • CT or MRI best to diagnose complications and diff diagnosis. • 6-8 weeks later colonoscopy if you want to rule out cancer.