Download

1 / 153
1.56k likes | 1.97k Vues
28. Endocrine Disorder. 부산백병원 산부인과 R4 서 영 진. Hyperandrogenism. Hirsutism : result of androgen excess → abnormalities of ovary, adrenal gland : increase expression of androgen effect Virilization : rare

E N D
28. Endocrine Disorder 부산백병원 산부인과 R4 서 영 진
Hyperandrogenism • Hirsutism : result of androgen excess → abnormalities of ovary, adrenal gland : increase expression of androgen effect • Virilization : rare indicates marked elevations on androgen caused by an ovarian or adrenal neoplasm
Hirsutism • Androgen ↑ : excessive growth of terminal hair • Pilosebaceous unit : androgen-responsive area transforms vellus hair (fine, nonpigmented, short) → terminal hair (coarse, stiff, pigmented, long) • Midline hair, sideburns, moustache, beard, chest, intermammary hair, inner thigh, midline lower back, intergluteal area
Androgen effects in hair vary in relation to specific regions of the body surface : no androgen dependence-lanugo, eyeblows, eyelashes : minimal sensitivity-limbs, trunk : sensitivity ↑- axilla, pubic region • Result from both increased androgen production & skin sensitivity :skin sensitivity–depend on local activity of 5α-reductase : 5α-reductase - testosterone → dihyhrotestosterone in hair follicles
Hair: cyclic activity – growth (anagen) involution (catagen) resting (telogen) : duration –according to body region, genetic factor age, hormonal effects • Hirsutism: relative > absolute, designation
Hypertrichosis and Virilization • Hypertrichosis: androgen-independent terminal hair (nonsexual area: trunk, extremities) - AD congenital disorder metabolic disorder (anorexia nervosa, hyperthyroidism) medication (acetazoamide, cirticosteroid, cyclosporine, diazoxide, interferon, minoxidil..) • Virilization: coarsening of the voice, increase muscle, clitoromegaly (width 3.4+1mm, length 5.1+1.4mm) feature of defeminization (loss of breast volume)
Focus on the age at onset & rate of progression : rapid- more severe degree of hyperandrogenism (ex. ovaran or adrenal neoplasm, Cushing synd.) : anovulation- probability of hyperandrogenism • Determining the extent of hirsutism : questions about shaving & use of depilatories : clinically mild, moderate, severe : scoring scale- adrogen-densitive hair in nine body scale of 0 to 4 → hirsutism > score 8
PCOS, congenital or adult onset adrenal hyperplasia, DM, cardiovascular disease, drug use • PEx: obesity, hypertension, galactorrhea, male-pattern baldness, acne, hyperpigmentation • DDX :Cushing syndrome
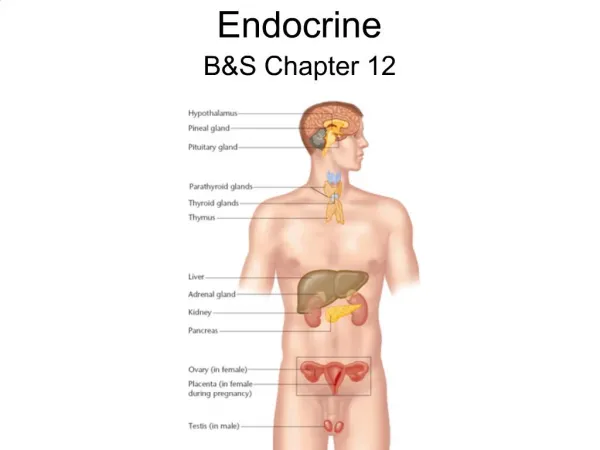
Role of Androgen • Androgen and their precusors : produced by both the adrenal glands and the ovaries : response to ACTH and LH
Adrenal 17-Ketosteroids : increases prepubertally : independent of pubertal maturation of H-P-O axis : adrenal steroid secretion- adrenarche : in adrenal cortex (zona reticularis) : growth of pubic hair, axillary hair and production of sweat by the axillary pilosebaceous units • Testosterone : 1/2 – peripheral conversion of androstenedione 1/2 – direct glandular (ovary, adrenal) secretion : 66~78%-binding sex hormone-binding globulin(SHBG) bologically inactive 20~32%-asssociated albumin 1~2%-unbound or free
: increases SHBG - high estrogen (pregnancy, luteal phase, use of estrogen) - thyroid hormone ↑, LC (→ reduced free testosterone) : decrease SHBG – free testosterone ↑ - androgenic ds(PCOS, CAH, Cushing) medication, growth hormone, obesity, hyperinsulinemia, pl]rolactin
Assessment of Hyperandrogenemia • Testosterone production ↑ ≠ total testosterone ↑ : because of depression of SHBG : moderate – normal range total testorterone : severe (virilization, neoplastic production of testosterone) - can be detected by measure of total testosterone : free testosterone level can be measured to assess increases in testosterone production
Free testosterone : standard technique- equilibrium dialysis but, expensive, complex, limited to settings : assessment of testosterone binding albiumin & SHBG AT = Ka [A] x FT AT- albumin-bound testosterone Ka – association constant of albumin for testosterone FT- free tetosterone A- albumin
The level of bioavailable testosterone : based on albumin, total testosterone, and SHBG • Testosterone → DHT (dihydrotestosterone) : active metabolite : by 5α-reductase · type I : skin · type II : liver, prostate, seminal vesicle, genital skin -type II>type I(20-fold higher affinity for testosterone) • the relative androgenicity of androgens : DHT = 300 testosterone = 100 androstenedione = 10 DHEAS = 5
Laboratory Evaluation • Bioavailable testosterone level (total testosterone, SHBG, and albumin level) Calculated free testosterone level • Most clinical situations : total testosterone, DHEAS, 17-hydroxyprogesterone
Normal values for serum androgens Testosterone (total) 20-80 ng/dL Free testosterone (calculated) 0.6-6.8 pg/mL Percent free testosterone 0.4-2.4 % Bioavailable testosterone 1.6-19.1 ng/dL SHBG 18-114 nmol/L Albumin 3,300-4,800 mg/dL Androstenedione 20-250 ng/dL DHEAS 100-350 μg/dL 17-OHP (follicular phase) 30-00 ng/dL
Hirsutism + absent or abnormal menstrual period : LH, FSH, prolactin, TSH • Hypothyroidism & hyperprolactinemia : reduce SHBG → unbound testosterone↑ → hirsutism • Cushing syndrome : 24hr urinary cortisol overnight dexamethasone suppresion test - 1 mg dexamethasone at 11:00 PM blood cortisol checked at 8:00 AM > 2 μg/dL → further workup
Total testosterone > 200 ng/dL : ovarian & adrenal tumor • DHEAS > twice the upper limit : adrenal hyperplasia : upper limit 350 μg/dL (9.5 nmol/L) • Virilization : total testosterone & DHEAS should be measured
Polycystic Ovary Syndrome(PCOS) • Most common cause of hyperandrogenism & hirsutism • Stein-Leventhal syndrome : amenorrhea + bilat. Polycystic ovaries + obesity • Principally oligomenorrhea or amenorrhea + clinical or laboratory evidence of hyperandrogenemia • Diagnostic criteria : Major – chronic anovulation hyperandrogenemia clinical signs of hyperandrogenism other etiologies excluded
: Minor – insulin resistance perimenarchal onset of hirsutism and obesity elevated LH-to-FSH ratio intermittent anovulation associated with hyperandrogenemia(free testosterone,DHEAS) • Hirsutism : 70% of PCOS in U.S.A 10~20% in japan → difference in skin 5α-reductase activity • Amenorrhea & oligomenorrhea • Obesity : 50% in PCOS insulin resistance hyperglycemia (type 2 DM)
Abnormal lipoproteins : total cholesterol. TG, LDL↑ : HDL, apoprotein A-I ↓ • Other finding : impaired fibrinolysis Hypertension atherosclerosis & cardiovascular disease MI
Pathology • Macroscopically, : 2 ~5 times the normal ovary : White, thickened cortex with multiple cyst • Microscopically, : superficial cortex- fibrotic and hypercellular prominent blood vessel : smaller atretic follicles : luteinized stromal cells
Pathophysiology and Laboratory Finding • By abnormalities in 4 endocrinologically compartment 1) the ovaries 2) adrenal glands 3) the periphery (fat) 4) the hypothalamus-pituitary compartment
The ovaries : most consistent contributor of androgen : dysregulation of CYP17(androgen-forming enzyme) : this hormone relates to ovarian androgenic activity 1. total & free testosterone level correlate directly with LH levels 2. more sensitive to gonadotropic stimulation, as a result of CYP17 dysregulation 3. GnRH agonist- suppresses testosterone and androstenedione levels 4. large dose of GnRH agonist are required for andro- gen suppression than endogenous gonadotropin- induced estrogen suppression
Testosterone level in PCOS : no more than twice the upper normal (20-80 ng/dL) : ovarian hyperthecosis- >200 ng/dL • Adrenal gland : hyperfunctioning CYP17 androgen-forming enzyme : DHEAS ↑ (50%) – hyeprresponsiveness to stimulation with ACTH
Peripheral compartment (skin & adipose tissue) 1. 5α-reductase in skin determines the presence or absence of hirsutism 2. fat cell: aromatase & 17β-HSD activity ↑ 3. with obesity, estrogen metabolism ↓ 4. E1 level ↑ : result of peripheral aromatization of androstenedione 5. E1 : E2 ratio ↑
Hypothalamic-pituitary compartment 1. LH pulse frequency ↑: the frequent observation of elevated LH & LH:FSH ratio 2. FSH : not increased with LH result from the combination of increased gonadotropin pulse frequency and synergistic negative feedback of elevated estrogen and normal ovary 3. prolactin ↑ : abnormal estrogen feedback to the pituitary gland
Insulin Resistance • Insulin resistance & hyperinsulinemia : ovarian dysfunction of PCOS : most common cause- obesity 1. Hyperinsulinemia is not a characteristic of hyperandrogenism in general but is uniquely associated with PCOS 2. in obese women with PCOS, 30-40% have glucose intolerance or DM, whereas ovulatory hyperandrogenic women have normal glucose tolerance and insulin PCOS-obesity: synergistic
3. Suppression of ovarian steroidogenesis with long– acting GnRH analogs in women with PCOS does not change insulin levels or insulin resistance 4. Oophorectomy in patients with hyperthecosis accompanied by hyperinsulinemia and hyperandrogenemia does not change insulin resistance, despite a decrease in androgen levels • Acanthosis nigricans : reliable marker of insulin resistance in hirsute women : thick, pigmented, velvety lesion- vulva, axilla, neck, breast, inner thigh
Acanthosis nigricans : reliable marker of insulin resistance in hirsute women : thick, pigmented, velvety lesion- vulva, axilla, neck, breast, inner thigh : testosterone >150 ng/dL fasting insulin > 25 μIU/mL Max insulin response to glucose load(75g)>300 μIU/mL
Screening strategies for diabetes and insulin resistance • Fasting glucose:insulin < 4.5 : insulin resistance • 2 hr GTT : nonobese(10%), obese(40-50%) with PCOS - inpared glucose tolerance, type II DM • testing women with PCOS for glucose intolerance is of value because their risk of cardiovascular disease correlates with this finding
Interventions • In obese, insulin–resistant women, caloric restriction that results in weight reduction will reduce the severity of insulin resistance (a 40% decrease in insulin level with a 10–kg weight loss) • Insulin resistance/hyperinsulinemia has been recognized as a cluster syndrome now called the metabolic syndrome or dysmetabolic syndrome X
Female waist >35 inches Triglycerides >150 mg/dL HDL cholesterol <50 mg/dL Blood pressure >130/85 mm Hg Fasting glucose: 110–125 mg/dL 2–hour GTT (75 g): 140–199 mg/dL
Ultrasonographic studies • Most important finding : bilateral increase in number if microcyst (0.5~0.8cm) : more than five microcyst in any imaging plane in each ovary : but, neither sufficiently sensitive nor specific finding
Long-term Risks • Chronic anovulation : persistently elevated estrogen, unopposed by progesterone increase the risk of endometrial carcinoma but, usually well-differentiated, stage I cure rates approaching 100% • Prevention of endometrial cancer : endometrial biopsy should be considered in PCOS : influence factor:- abnormal bleeding, weight ↑, age
Hyperestrogenic state : breast cancer, ovarian cancer ↑ (2-3 fold) : the risk is greater in nonobase women, not taking oral contraceptives
Treatment of Hyperandrogenism and PCOS • Depends on a aptient’s goals : hormonal contraception, ovulation induction, et al : ovulatory dysfuction progestational interruption of unopposed estrogen effects on endometrium is required • Interruption of hyperandrogenism & control of hirsutism : can be accomplished simutaneously : if patient desires pregnancy, control of hirsutism may not be possible
Weight Reduction • The initial recommendation : reduce insulin, SHBG, and androgen : restore ovulation with ovulation-induction agents • Weight loss of as little as 5~7% : reduce bioavailable or calculated testosterone : restore ovulation & fertility in more than 75% women
Oral Contraceptives • Combination OCs : decrease adrenal & ovarian androgen production : reduce hair growth in 2/3 hirsute patients 1. progesterone component- LH ↓ androgen production ↓ 2. estrogen- increase hepatic production of SHBP free testosterone ↓ 3. circulating androgen ↓ 4. by inhibition of 5α-reductase - decrease conversion of testosterone to DHT in skin
When use OCS, a balance must be maintained between the decrease in free testosterone levels and the intrinsic androgenicity of the progestin : progestin (norgesterol, norethindrone, norethindrone acetate) - androgenic activity ↑ - new progestin (desogestrel, gestodene, norgestimate, grospirenone)
Medroxyprogesterone Acetate • Directly affects the hypothalamic-pituitary axis by decreasing GnRH production and release of gonadotropin reduce testosterone & estrogen production in ovary • Oral: 20~40 mg daily IM: 150 mg every 6 weeks to 3 months • Side effects: amenorrhea, bone density ↓, depression, headache, hepatic dysfunction, Wt. gain
Gonadotropin-releasing Hormone Agonist • Allow the differentiation of androgen produced by adrenal sources from that of ovarian sources • GnRH agonist : suppress ovarian steroids • Leuprolide acetate IM every 28 days : decrease hirsutism & hair diameter • + OCs or estrogen replacement : prevent bone loss, menopause side effect
Glucocorticoids • Dexamethasone : treat adrenal or mixed adrenal and ovarian hyperandrogenism • 0.25 mg nightly or every other nightly : suppress DHEAS (<400 μg/dL) • 40 times the glucocorticoid effect of cortisol : if daily over 0.5 mg, adrenal suppression & Cushing syndrome : maintain morning cortisol level (>2 μg/dL) • Reduce hair growth rate & acne
Ketoconazole • Inhibits the key steroidogenic cytochromes • 200 mg/day : reduce androstenedione testosterone calculated free testosterone
Spironolactone • Effective K sparing diuretics for treatment of HTN • Antagonist of aldosterone : competitively binds to aldosterone receptors in the distal tubular region of the kidney 1. competitive inhibition of DHT at intracellular receptor 2. testosterone biosynthesis ↓ by a decrease in the CYP 3. androgen catabolism ↑ 4. inhibition of skin 5α-reductase activity
Using at least 100 mg daily for 6 months : most common dosage- 50~100 mg twice daily : reduce sexual hair, hair diameter, hair volume • Side effect : menstrual irregularity (metrorrhagia) : mastodynia, urticardia, scalp hair loss • Not recommended : renal insufficiency, hyperkalemia : check K, Cr level
Cyproterone Acetate • Synthetic progestin : antiandrogenic properties : competitive inhibition of testosterone, DHT at the level of androgen receptor : hepatic enzyme ↑- androgen clearance ↑ • + ethinyl estradiol : reduce testosterone, androstenedione suppress gonadotropin increase SHBG
Reverse sequential regimens : cyproterone acetate 100 mg/day on days 5 to 10 ethinyl estradiol 30-50 mg/day on days 5 to 26 • Side effect : fatigue, Wt. gain, libido ↓, nausea, headache, irregular bleeding