Download
1 / 40
410 likes | 885 Vues
Overview . Introduction Risk factors Clinical manifestationModification of risk factors Antiplatelet Rx Exercise Rx for claudication Drug Rx for claudication Conclusion . Introduction . PAD caused by atherosclerotic occlusion of arteries to legs Prevalence 12% and increases to 20% if person

E N D
2. Overview Introduction
Risk factors
Clinical manifestation
Modification of risk factors
Antiplatelet Rx
Exercise Rx for claudication
Drug Rx for claudication
Conclusion
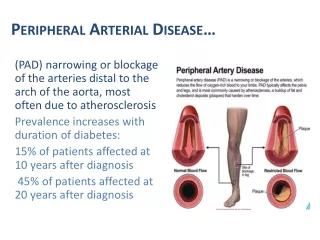
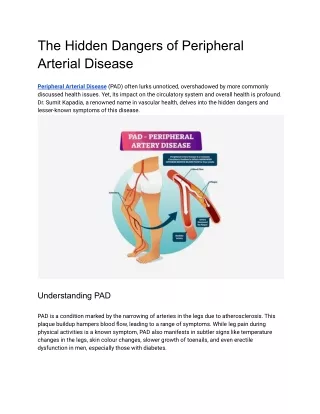
3. Introduction PAD caused by atherosclerotic occlusion of arteries to legs
Prevalence 12% and increases to 20% if persons older than 70 yr.
Affects men and women equally
pt. with PAD , even absence of Hx of MI or ischemic stroke have same relative risk of death from CVS cause as pt. with Hx of CAD or CVD
4. Introduction Rate of death of all causes equal in men and women and is elevated even in asymptomatic pt.
Severity of PAD is closely associated with risk of MI , ischemic stroke , and death from vascular cause
Lower ABI � greater risk of CVS events
Critical leg ischemia � mortality of 25%
6. Introduction Claudication = walking induced pain in one or both legs [primarily affecting calves] does not go away with continued walking , relieved by rest
Present in 15-40% of PAD
Associated with diminished ability to perform ADL
7. Risk factors Older age [>40 yr.]
Smoking
DM
Hyperlipidemia
HT
Hyperhomocysteinemia
8. Clinical manifestations 1/3 have typical claudication
In pt. with claudication , severity increases slowly : 25% worsening claudication
: 5% undergo amputation within 5 yr.
: 5-10% have critical leg ischemia
[ischemic pain in distal foot , ischemic ulceration , or gangrene]
9. Clinical manifestations > 50% of pt. identified as PAD on ABI do not have typical claudication , but have other types of leg pain on exertion � with reduced activity and quality of life
11. Modification of risk factors Smoking cessation
Rx of hyperlipidemia
Rx of DM
Rx of HT
Additional approach
12. Smoking cessation Slow progression to critical leg ischemia and reduces risk of MI and death from vascular causes
Not certain that smoking cessation reduces severity of claudication
From meta-analysis : did not improve MWD
13. Rx of hyperlipidemia Statin not only lower serum cholesterol concentration , but can improve endothelial function
Lipid-lowering Rx has benefit in PAD , who often coexisting CAD and CVD
Target : serum LDL< 100 mg/dl
serum TG < 150 mg/dl
14. Rx of DM Intensive control BS prevents microvascular complications , but its effect on macrovascular complications is less certain
From UKPDS : intensive drug Rx � trend toward a reduction in MI but had no effect on amputation due to PAD
Intensive BS control in type 1,2 DM � may not favorably affect PAD
15. Rx of HT Data are not available to clarify whether Rx will alter progression of disease or risk of claudication
BB : from meta-analysis , BB are safe in pt. with PAD , except in most severe affected pt.
ACEI , from HOPE : death from vascular causes , nonfatal MI or stroke did not differ significantly between pt. with PAD and no PAD
16. Additional approach High serum homocysteine = independent risk factor for PAD and increases risk of death from CVS causes
B vitamins and folate lower serum homocysteine concentration
Despite ease of Rx , no clinical trials demonstrating benefit in pt. with PAD
17. Additional approach Estrogen Rx reduces several CVS risk factors in postmenopausal women
Estrogen has no role in Rx of PAD in postmenopausal women
Presence of PAD is not contraindication to estrogen Rx in women with indication
Estrogen has been associated with reduce graft patency in women undergo femoropopliteal bypass Sx
18. Antiplatelet Rx In pt. with cardiovascular disease : antiplatelet reduce risks of nonfatal MI , ischemic stroke and death from vascular causes
Support use of antiplatelet in pt. with PAD
19. ASA FDA expert panel found insufficient evidence to approve ASA as indicated for pt. with PAD
ASA may favorably affect peripheral circulation : from Physicians� Health Study [1st prevention trial] , ASA reduced subsequent need for peripheral arterial Sx
20. ASA High dose ASA [600-1500 mg/d] as effective as low dose ASA [75-325 mg/d]
ASA alone as effective as combination of ASA and dipyridamole , sulfinpyrazone or ticlopidine in prevent graft occlusion
21. Ticlopidine [Ticlid] In PAD , ticlopidine more effective than placebo in reducing risk of fatal or nonfatal MI or stroke
Ticlopidine may reduce severity of claudication and need for vascular Sx
Risk of thrombocytopenia , neutropenia [2.3%] and TTP [1:2000-4000]
22. Clopidogrel [Plavix] Fewer hematologic side effects than ticlopidine
FDA approval clopidogrel for 2nd prevention of atherosclerotic events in pt. with atherosclerosis , include PAD
Report of TTP = 4:1000000
23. Summary for antiplatelet drug Although data are not conclusive , ASA should be considered 1st antiplatelet drug for preventing ischemic events in PAD
ASA also effective in maintain vascular graft patency and may prevent thrombotic complications of PAD
FDA approval clopidogrel for prevent ischemic events in PAD and may be more effective than ASA
24. Exercise Rx for claudication Demonstrated in > 20 randomized trials : exercise improves MWD , QOL , and community-based functional capacity
Rigorous exercise training program may be as beneficial as bypass Sx and may be more beneficial than angioplasty
Meta-analysis , exercise training increased MWD 179 m.
25. Exercise Rx for claudication Greatest improvements in walking ability occurred when each exercise session > 30 min , at least 3 times/wk , pt. walked until near maximal pain was reached and program lasted 6 mo or longer
Time course of response to exercise program not been fully established , benefit observed as early as 4 wk
26. Exercise Rx for claudication Exercise improved maximal walking time 150%, exceeded than medication [pentoxifylline 20-25% , cilostazol 40-60%]
Several limitations : require a motivated pt. in supervised setting
27. Drug Rx for claudication Vasodilator drugs
Pentoxifylline [Trental]
Cilostazol [Pletal]
Naftidrofuryl [Praxilene]
Levocarnitine and propionyl levocarnitine
Prostaglandins
28. Vasodilator drugs Papaverine [1st medication studied for claudication] ; no evidence of clinical efficacy of drugs of this class
Vasodilators do not affect stenosed/occluded vv. that dilate/constrict due to endogenous factors , but may decreased resistance in other vv.
Vasodilators can lower systemic pressure = reduction in perfusion pressure
Current data do not support use of vasodilators for claudication
29. Pentoxifylline Methylxanthine derivative that improve deformability of RC and WC , lower plasma fibrinogen concentration and has antiplatelet effect
Meta-analysis : net benefit 44 m. in MWD , may have small effect on walking ability , insufficient to support its widespread use
30. Cilostazol FDA approved in 1999 for Rx claudication
Inhibit phosphodiesterase type 3 � increase intracellular concentration of c-AMP
Inhibits platelet aggregation , formation of arterial thrombi , vascular smooth muscle proliferation and cause vasodilatation
Extensive hepatic metabolism : CYP3A4 , drug that inhibit CYP3A4 may increase serum cilostazol concentrations
31. Cilostazol 4 RCT : improve both pain free and MWD , compared with placebo
3 RCT : improve several aspects of physical functioning and QOL
Causes small increase in ABI and serum HDL concentration
Side effect : headache [34%] , transient diarrhea , palpitation and dizziness
32. Cilostazol Can be administered with ASA , no data on safety of coadministration of cilostazol with clopidogrel
Cilostazol should not be given to pt. with claudication who also have HF
33. Naftidrofuryl Antagonism of 5-hydroxytryptamine receptors
Improve pain free but not MWD
Not available in USA
34. Levocarnitine and propionyl levocarnitine In PAD : metabolic abnormalities develop in skeletal muscles [impairment of activity of mitochondrial electron transport chain in ischemic muscle and accumulation of intermediates of oxidative metabolism =acylcarnitine]
Claudication caused not just by reduced blood flow but also by metabolism alteration
35. Levocarnitine and propionyl levocarnitine Drug may improve metabolism and exercise performance of ischemic muscle
Improve MWD and QOL
Not been approved for use in USA
36. Prostaglandins Evaluated primarily for Rx critical leg ischemia , but fewer studies in claudication
PGE1 and beraprost improve MWD and QOL
Side effect : headache , flushing and GI intolerance
Use of PG in PAD need further evaluation
37. Conclusion PAD should be considered candidate for 2nd prevention strategies , just as CAD
Antiplatelet : effective in reduce risk of fatal and nonfatal ischemic events in PAD
ASA should be considered in all pt. , with clopidogrel an alternative [potentially more effective drug]
38. Conclusion Walking-based exercise program considered first for all pt. with claudication
Cilostazol improve both pain free ,MWD and QOL
39. When should a pt. be referred to a vascular surgeon ? Pt. has unacceptable symptoms despite appropriate Rx
Pt. has weak or absent femoral pulse
Pt. with critical limb ischemia [rest pain , gangrene , or ulceration] should be referred urgently
40. Available drug in Siriraj Hospital
41. References Medical treatment of peripheral arterial disease and claudication : NEJM Vol.344 , No.21 , May 2001
Exercise training for claudication : NEJM Vol.347 , No.24 , December 2002
Management of peripheral arterial disease in primary care : BMJ Vol.326 , March 2003
Diabetes and vascular disease : Circulation 2003;108:1655-1661
Secondary prevention of peripheral vascular disease : BMJ Vol.320 , May 2000