Download
1 / 47
480 likes | 631 Vues
Current Criticism on IVM Treatment. Dr. Milton Leong MDCM DSc (McGill) Director, IVF Center , Hong Kong Sanatorium & Hospital Specialist in Reproductive Medicine Adjunct Professor, OBS-GYN, McGill University. 1. Current Criticism of IVM. Lower fertilization rate

E N D
Current Criticism on IVM Treatment Dr. Milton LeongMDCM DSc (McGill) Director, IVF Center, Hong Kong Sanatorium & Hospital Specialist in Reproductive Medicine Adjunct Professor, OBS-GYN, McGill University 1
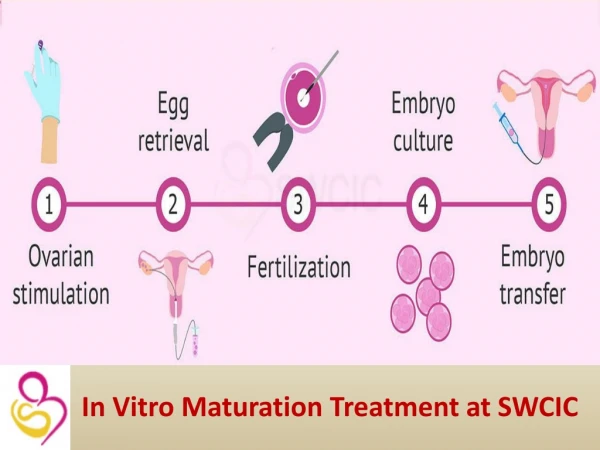
Current Criticism of IVM Lower fertilization rate Lower pregnancy & implantation rates Higher pregnancy loss Inadequate neonatal and postnatal data Possible genetic and epigenetic changes
Current Criticism of IVM Inconsistent pregnancy rates Inconsistent clinical details regarding timing, endometrium, EC techniques Inconsistent laboratory details regarding EC, culture system and culture techniques Inertia from IVF success vs “experimentation”
Current Status of IVM Like IVF 25 years ago, IVM is a treatment tool waiting to be universally applicable. At the moment, there is some sort of alchemy bias. There are also unresolved issues, like IVF then, that needs to be clarified.
Current Status of IVM • IVM is a CONCEPT • IVM is a laboratory technique, not a stand alone treatment modality • IVM is a method of preparing oocytes so IVF can be carried out • IVF/M have its advantages over conventional IVF in some patients • IVM can enable IVF to be performed when otherwise it is impossible
Current Status of IVM Similar to IVF in 80’s, issues regarding IVM: • Technical - timing of EC aspiration technique drugs to use • Laboratory - culture system • Outcome - now there is IVF to compare • Safety - baby registry long term genetic changes
Progress in IVM • Edwards 1965 : 1st in vitro matured oocyte • Veeck 1983 : 1st IVM pregnancy from an ovum derived from a • stimulated cycle • Cha et al. 1991 : the first pregnancy from in-vitro matured oocytes derived from a caesarean section donor • Trounson et al. 1994: IVM in women with PCOS • improvements in culture condition and transfer techniques have demonstrated that IVM is an effective treatment for women with PCO or PCOS. • In general, clinical pregnancy and implantation rates for infertile women with PCO or PCOS have reached approximately 30-35% and 10-15%, respectively, (Chian et al., 2004).
Advantages of IVM • No/minimal stimulation: less OHSS less long term effect safety factor – cancer patients • Flexible start time, no preparation • Cancer patients no theoretical and actual risk (especially breast ca) can treat anytime
Indications for IVFM treatment • Polycystic ovaries (PCO) or polycystic ovary syndrome (PCOS) (primary); • Hyper responders for gonadotropin stimulation (alternative); • Delayed responders for gonadotropin stimulation (alternative);
PCOS and IVF • Pregnancies were comparable to non-PCOS patients • Lowered fertilization rate • Increased miscarriage rate • FSH requirement leads to under or over response • Higher cancellation rate • Much higher chance of OHSS
PCOS, OHSS and IVF • Risk up 5-30 fold (6-30%) • Estradiol >3000pg/ml • # Follicles >20
OHSS in PCOS Undergoing IVF • Preventive Measures: • Pre-treat with laparoscopic drilling • Use GnRH-ant then GnRH-a to trigger • Metformin (as short as 28 days) • No Transfer, Cryopreservation • Early Aspiration of Follicles - 2 operations • Conversion to IVM • IVM with and/or without stimulation
GnRHav.s. HCG in IVF-IVF used in PCOS 300 ųg Buserelin vs 10000 unit HCG Maturation rate same (±50%) Fertilization rate same 85% Pregnancy rate same 41% OHSS rate < 1% A. Fukuda et al, Fertility and Sterility 2008
IVM/IVF vs IVF for PCOS Child TJ, et al,2002
IVM-IVF in POS 210 cycles 1883 oocytes 56% maturation 83% fertilization Pregnancy rate 31% fresh 32% frozen-thawed 50/56 pregnancies delivered Miscarriage 11% A. Fukuda et al, Fertility & Sterility 2008
McGill IVM results by age group (own oocytes only – patients with PCOS)
Updated IVM success rates • Clinical pregnancy rate 30-35% per ET; • Implantation rate 9-15% per ET; • More than 1,000 healthy live births;
Pregnancy Outcome in IVM Malformation: Cha, Fertil. Steril. 2005 5,3% major malformation rate Later neuromotor development: Soderstrom-Anttila, Hum. Reprod. 2006 ))) Minor developmental delay at first year ))) No Difference in the second year
Outcome of IVM, IVF, ICSI and normal pregnancies • obstetrical and perinatal outcome of 432 babies (55 IVM, 217 IVF, 160 ICSI) compared with 1,296 age-matched spontaneous pregnancies (controls) delivered at a single hospital (MUHC) Buckett et al. Obstet Gynecol 2007; 110:885-91
Relative risk for any congenital abnormality compared with controls
Pregnancy Outcome in IVM • Mikkelsen et al. (2005) ----- 47 IVM babies • 2 twins • 1 NT Normal karyotype • 2 preterm deliveries • 1 stillbirth (42 weeks) • 1 chromozomal abnormality
Drawbacks in IVM Lower development competence Lower blastocysts formation Lower implantation rate Lower pregnancy rate Higher miscarriage rate But, where is the beef? 27
Development Competence of Oocytes Nuclear maturation – progression to Meta phase II stage. Cytoplasmic maturation – coordinated arrangement of proteins, organelles. Gosden R et al, Bioessays 1997 Nogueira D et al, Fertil Steril 2007 28
Development Competence of Oocytes IVM results in asynchronous nuclear vs. cytoplasmic maturation IVM (mouse oocytes) showed different spindle morphology when assessed with immuncytologic staining. Combelles CM et al, Human Reprod 2002 Sanfins A et al, Biol Reprod 2003 29
Does size matter In vivo matured oocytes > immature. Maturation rate (IVM) related to diameter of oocytes. Zona thickness, total oocytes + zona diameter has no correlation. Cavilla JL et al, Human Reprod 2008 31
Outcome of IVM In mouse, in vitro vs. in vivo maturation. In vitro: a) established optimized culture fluid b) no amino acid culture fluid Comparing life span, and variety of physiological and psychological tests. No difference between in vitro or in vivo life span or behavior. In culture fluid a) reduction in cardiac output and pulse rate. Eppig JJ et al, Human Reprod 2009 32
Outcome of IVM 21 children IVM vs. non IVM, age 2-5 PE – neurological examination and developmental (Bayley Scales) Findings: Normal Karyotype, Normal PE Mean Mental Developmental Index Score 92.7% vs. 97.2%, Mean Psychomotor Development Index Scores 96.7% vs. 96.2%. Conclusion: No developmental delay in infancy and early childhood Shu-chi M et al, Early Hum Dev 2006 33
Outcome in IVM 46 children assessed at 6, 12, 24 months Muenchener Funktionelle Entwicklungs Diagnostik and Bayley Scales 6 mths Normal 12 mths 19% IVM expressed minor developmental problem 1/43 had optic glioma 24 mths Normal development Suikkari M et al, Human Repro 2006 34
Outcome of IVMIVM vs. IVF vs. ICSI Buckett WM et al, Fertil Steril 2008 35
IVM outcome High miscarriage rate may be due to other causes (endometrium?) because cytogenetic and DNA fragmentation analysis of the aborted embryos were not different from routine IVF. Benkhalifa Meta, Reprod Biomed Online 2009 36
Genetics in IVM Methylation of the KCNQ1OT1 gene in vitro matured oocytes methylate DNA the same as GV and mature genes. At 28 hours of culture, however, GV and MI oocytes from natural cycles significantly methylate more than those from stimulated cycles. ?Hyperstimulation recruits too young follicles Khoueiry R, J Med Genet 2008 37
Genetics in IVM No difference in meiotic spindle organization, chromosome alignment and aneuploidy (mouse oocytes) Xu L et al, Syst Biol Reprod Med. 2008 38
Genes and IVM Rhesus Monkey oocytes IVM vs. VVM Only 56 mRNA’s differentially expressed. These are related to cell homeostasis, cell-cell interactions, cell adhesion, mRNA stability and translation. Over expression of maternal genes. IVM oocytes can be very close to VVM oocytes but interruption of normal oocyte-somatic cell interaction may disturb full developmental competence. Lee YS et al, Physiol Genomics 2008 40
Genes and IVM IVM, then examine GV, MI, MII oocytes, using H19. Differentially methylated region GV Unmethylated MI Arrested – altered methylation pattern MII 15/20 normal unmethylated pattern 5/20 methylated pattern Risk of epigenetic changes so safety of IVM should be assessed. Borghol N et al, Genomics 2006 41
Genes in IVM Although in vivo maturated an in vitro maturated oocytes has very similar gene expression, the major difference is in persistence of immature genes. IVM oocytes differs in gene expression related to cytoplasmic function and cellular storage and homeostasis. Well D et al, Am J Obstet Gynecol. 2008 42
IVM successes PCOS patients Natural cycle IVF/M Birth after vitrification Repeated successful pregnancies in same patients Birth after preservation of oocytes for cancer patients McGill Reproductive Centre 43
Conclusions • IVM is efficient infertility treatment, • especially for patients with PCO/PCOS; • IVM provides an alternative for some patients during ovarian stimulation cycles.
Conclusions • IVM simplifies treatment, reduces costs and eliminates OHSS • IVM successful in women with high AFC • hCG increases final number of MII oocytes and rate of maturation • IVM may be helpful in women with repeated poor embryo quality in previous IVF cycles for no obvious reason, or repeated poor responders to ovarian stimulation
Conclusions • IVM produces CPR/C of 35%, and up to 48% in selected cases, in women up to 35 . • obstetric and perinatal outcomes of IVM pregnancies comparable with IVF and ICSI • IVM may be useful for oocyte donation or PGD • IVM may offer a chance for fertility preservation to young women with cancer and undergoing cytotoxic treatment. • IVM may not replace standard IVF but appears to play increasingly important role in ART
Current Status of IVM An established treatment for PCO/PCOS In experienced hands closing on IVF Needs registry outcome and follow up Some animal data regarding genetic changes May be epigenetic changes All can be solved by proper practice and follow up and large data collection as in REGISTRY