Download
1 / 23
240 likes | 367 Vues
An Interesting Case of Thoracic Outlet Syndrome. Laurel Romer, M.D. Primary Care Conference May 14, 2008. Financial Disclosure. I have received no outside financial support for this presentation. Learning Objectives. Understand the pathophysiology of TOS

E N D
An Interesting Case of Thoracic Outlet Syndrome Laurel Romer, M.D. Primary Care Conference May 14, 2008
Financial Disclosure • I have received no outside financial support for this presentation.
Learning Objectives • Understand the pathophysiology of TOS • Learn the provocative maneuvers to diagnose TOS • Understand treatment options for TOS
Outline • Case Presentation • Definition • Anatomy • Epidemiology • Differential Diagnosis • Symptoms • Physical Exam • Diagnostic Testing • Treatment • Case Presentation
Case Presentation • EB is a 30 year old white female who presents with left upper extremity swelling and pain, which began while she was watching a movie in a theater. She says that when she left the movie, a couple of hours after the symptoms initially began, she noted that the swelling of her left arm was worse and there was pain in her shoulder region. She also could not get her ring off of her finger and her left hand was dusky. She did not have any shortness of breath or pleuritic chest pain. A few days before that the patient had been shoveling snow during a heavy snow storm and the day after that developed upper respiratory symptoms including sore throat, sharp chest pain, a sensation of her ears being plugged and swollen glands in her neck.
Case Presentation • The patient had a Doppler evaluation which revealed clot in the subclavian and axillary veins. A CT scan of the chest revealed no evidence of pulmonary embolism. She had a hypercoagulable workup which was negative. She was treated with heparin and then started on Coumadin and consideration was given a couple of times to giving thrombolytics but this was not done. She was taken off her OCP.
Case Presentation • Ultrasound of the left upper extremity was performed about 15 days after the onset of symptoms and revealed interval partial recanalization of the left subclavian vein and slight increase in flow within the left axillary vein in a patient with previous occlusive thrombus in these vessels. • MRI of the left upper extremity was performed to look for a compressive component to her vasculature in the left upper extremity as a cause for the DVT.
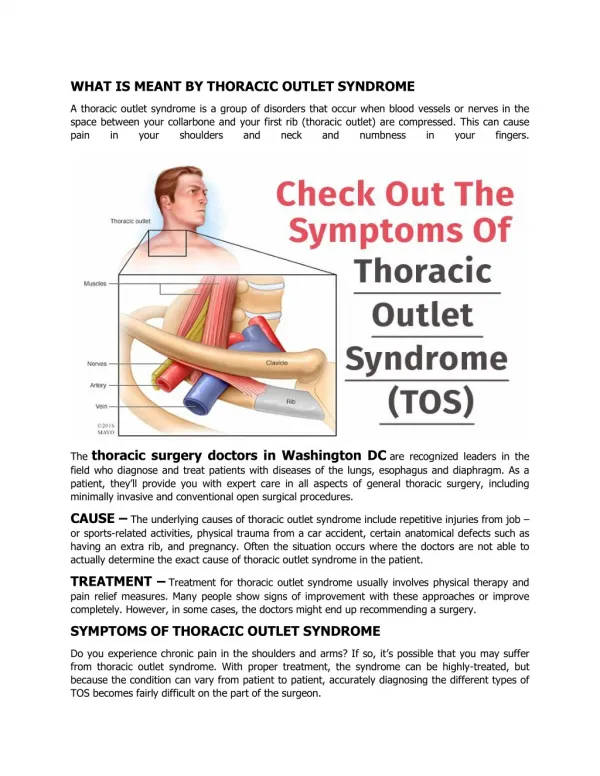
TOS - Definition • Adson first described his maneuver in 1927 • Thoracic Outlet Syndrome first coined in 1956 • Upper extremity symptoms due to compression of the neurovascular bundle by various structures in the area just above the first rib and behind the clavicle • Etiologies include congenital bony structures, fibromuscular abnormalities, posture, certain movements, trauma
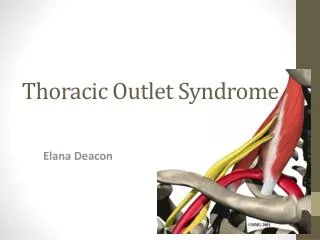
TOS - Anatomy Google Images
TOS - Epidemiology • 3 to 80 cases per 1000 • Ages 20-40 • Women > Men (4:1) • Neurogenic TOS (90%) > Venous TOS > Arterial TOS (<1%) • Cervical ribs occur in < 1% of population • 70% women
TOS – Differential Diagnosis • Cervical disc disease • Cervical facet disease • Malignancies (Pancoast/local tumors, spinal cord tumors) • Peripheral nerve entrapments (ulnar or median nerve) • Brachial plexitis • Rotator cuff injuries • Fibromyalgia, muscle spasm • Neurologic disorders (MS) • Chest pain, angina • Vasculitis • Vasospastic disorder (Raynaud’s) • Neuropathic syndromes of upper extremity Talu, GK: Agri 17 (2005), 5-9.
TOS - Symptoms • Neurogenic TOS • Pain, paresthesia, and weakness in the hand, arm and shoulder, plus neck pain and occipital headaches • Raynaud’s phenomenon, hand coldness and color changes are also seen frequently in NTOS Sanders RJ, et al. J Vasc Surg, 46(3), 2007, 601-604.
TOS - Symptoms • Venous TOS • Swelling of the arm, plus cyanosis is strong evidence of subclavian vein obstruction • Pain often present, but may be absent • Arm swelling distinguishes VTOS from ATOS and NTOS Sanders RJ, et al. J Vasc Surg, 46(3), 2007, 601-604.
TOS - Symptoms • Arterial TOS • Digital ischemia, claudication, pallor, coldness, paresthesia and pain in the hand (but rarely in the shoulder/neck) • Symptoms are a result of arterial emboli from a mural thrombus in a subclavian artery aneurysm or from thrombus forming distal to subclavian artery stenosis Sanders RJ, et al. J Vasc Surg, 46(3), 2007, 601-604.
TOS – Physical Exam • VTOS • arm swelling • cyanosis • distended superficial veins over the shoulder and chest wall • NTOS • Tenderness over scalene muscles • Positive provocative tests Sanders RJ, et al. J Vasc Surg, 46(3), 2007, 601-604.
TOS – Physical Exam • Provocative tests • Adson test • Neck rotation and head tilting (ear to shoulder) eliciting pain and paresthesia down the contralateral side • 90°AER - Abducting arms to 90 degrees in external rotation, brings on symptoms within 60 seconds • Upper Limb Tension Test Sanders RJ, et al. J Vasc Surg, 46(3), 2007, 601-604.
CLOSE Fig. Upper Limb Tension Test (ULTT). Position 1: Arms abducted to 90° with elbows extended. Position 2: Dorsiflex wrists. Position 3: Tilt head to side, ear to shoulder. Each maneuver progressively increases stretch on the brachial plexus.
TOS – Diagnostic Testing • Neck or chest xray • Detects cervical rib or elongated C7 transverse process • EMG/NCS • Normal in large majority of clinically + NTOS • Most common finding in NTOS is ulnar neuropathy • Recent study suggests NCV abnormalities of the sensory medial antebrachial cutaneous nerve are seen in NTOS • MRI/CT • Venography/venous duplex • VTOS • Arteriography • Only indicated in ATOS Seror, O. Clin Neurophysiol 115 (2004), 2316-2322.
TOS – Treatment • Conservative Management • Massage, hydrotherapy and PT • Behavioral modification/avoidance of provocative activities • PT to strengthen muscles of the pectoral girdle and restore normal posture • Improvement: 50-90%
TOS – Treatment • Definitive management • Surgical decompression of the neurovascular bundle • First rib resection • Scalenectomy • Subclavian artery reconstruction • Cervical sympathectomy
Case Presentation • A few months later, venous duplex ultrasound appears normal. There is no evidence of impingement on either side. Both veins are patent by duplex but there is bilateral impingement in multiple stress positions on both the right and left side.
Case Presentation • EB met with a vascular surgeon who felt that she was at high risk for recurrence of BUE DVT (off anticoagulants) without definitive treatment • A left 1st rib resection was performed • A few months later a right 1st rib resection was performed • She was taken off anticoagulants • She was restarted on her OCP along with Aspirin 81mg qd • She was strongly advised to continue longterm with a shoulder girdle strengthening exercise program
References Barkhordarian, S. J Hand Surg 32 (4/2007), 565-570. Demondion, X, et al. Radiographics 26 (2006), 1735-1750. Sanders RJ, et al. J Vasc Surg, 46 (2007), 601-604. Seror, O. Clin Neurophysiol 115 (2004), 2316-2322. Talu, GK: Agri 17 (2005), 5-9. Vanti C, et al. Eura Medicophys 43 (2007), 55-70.