Download
1 / 18
200 likes | 261 Vues
Benign prostatic hyperplasia BPH. *BPH is the most common benign tumor in men. *Its age related disease. For Pathololgy mean cellular proliferation of stromal and epithelial elements of prostate For Radiologist mean an enlarged prostate > 30cm

E N D
*BPH is the most common benign tumor in men. *Its age related disease. For Pathololgy mean cellular proliferation of stromal and epithelial elements of prostate For Radiologist mean an enlarged prostate > 30cm For Urologsit represent acollection of lower urinary tract symptoms (LUTs) that develop in male population in association with aging and prostatic enlargement Pathology. The prostate composed of -stroma (smooth muscle & fibrous tissue) and -epithelium. BPH can arise from any one of them or in combination
Etiology. BPH need both Age +Androgen to develop • Increase in cell number • Epithelial and stromal proliferation. • Impaired programmed cell death (apoptosis) • Proposed factors that play role in aetiology include • Androgens • Estrogens • Stromal-epithelial interactions • Growth factors • Neurotransmitters • Genetic(autosomal dominant) family history usually effect younger age group
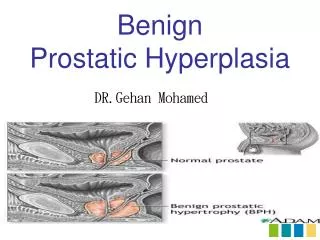
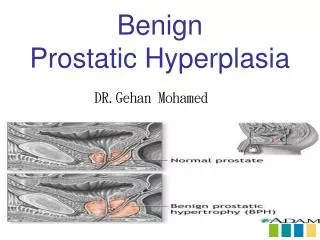
Anatomically the prostate had 3 zones -peripheral (70%) commonest site for Ca, -central (25%) around ejaculatory duct, & -transitional (5%) periurethral. BPH uniformly originate from the transitional zone & as the nodule enlarge compress the outer zones of the prostate resulting in surgical capsule. Pathophysiology Increaseurethral pressure lead tobladder wall hypertrophy so First : the changes that lead to decrease compliance causing frequency and urgency
Second :changes associated with decreased contractility causing decrease force of urinary stream,hestancy,intermittency and increase resudial volume Clinical features Either obstructive or irritative. obstructive symptoms -hesitancy, -decrease force & caliber of stream, -sensation of incomplete bladder emptying, -double voiding -straining to urinate, & post void dribbling.
Irritative symptoms urgency, frequency, & nocturia. * The amount of post void residual urine is extremely variable in sequential evaluation of same patient. DRE, used to determine the size, consistency of the prostate -a smooth firm usually BPH while -induration signify the possibility of Ca & need further evaluation.
-retention may occur usually precipitated by prostatic infection or infarction, ingestion of diuretic, anticholenergic, antidepressant • Symptom not related to prostatic size • Investigation • GUE, infection & hematuria. • Renal function : b.urea & s.creatinine. • PSA : is optional .prostatic tumor marker • Imaging : IVU &U/S is some time recommended. • Cystoscopy. Used to choose surgical approach when surgery is indicated.
D.Dx. Obstructive condition of lower tract like -urethral stricture, -bladder neck contracture, -bladder stone, & -Ca prostate. irritative -UTI, -CIS, & -neurogenic bladder
Treatment Options • Watchful waiting • Medication • Surgical approaches TURP Invasive open procedures Minimal invasive A-Watchful waiting Idea is only 5% of BPH patients will develop retention • Mild symptoms with not very active life style • Follow up every 3-6 months • Offer suggestions that reduce symptoms Like avoid caffeine , night time excessive fluid and decongestant,antihistamine anticholinergic
B-Medical therapy. 1-Alpha blocker: The human prostate & bladder neck contain alph-1a receptors. Alpha blocker lead to smooth muscle relaxation & dilatation of bladder neck. Alpha blocker either nonselective act on alpha like phenoxybenzamine Selective which either short acting e.g prazosin or, long acting e.gterazosin & doxazosin . These need dose titration to decrease their side effect
side effect include -orthostatic hypotension, -dizziness, -tiredness, -retrograde ejaculation, -rhinitis, & -headach . Highly selective act on alpha 1a receptors like Tamsolusin and Silodosin in both no need for dose titration because it had fewer side effect.mostly causing retro grad ejaculation
2- 5-alpa reductase inhibitor Finasteride and dutasteride are 5 alpha reductase inhibitors that block the conversion of testosterone to dihydrotestosteron. This drug act on epithelial component (adenoma) of the prostate reduce the size of the gland (20% reduction of weight in 6 months). side effect -decrease libido & -reduce PSA level to 50% complicating cancer detection.
B-Surgical management. Absolutetely Indicated in 1-refractory retention (after at least 1 trial of catheter removal), 2-recurrent UTI due to PBH 3-recurrent gross hematuria, due to PBH 4-bladder stone, 5-renal insufficiency 6-bladder diverticulum 7- failure of medical treatment (medication not improving the quality of life) *provide these are from BPH.
1-TURP (transurethral resection of the prostate) -resection of the prostate endoscopically into small pieces which removed by bladder wash. -Used in 95% of BPH. complications. Immediate -Bleeding -Capsular perforation with fluid extravasation -Infaction -TURP syndrom resulting from hypervolemic hyponatremic state due to absorption of hypotonic irrigating solution. Manifested by nausea, vomiting, confusion, hypertension, bradycardia,& visual disturbance
Late complication • Urethral stricture • Bladder neck contracture • Retrograde ejaculation • Impotence • Incontinence
2-open simple prostatectomy. Indicated when TURP not performed due to 1- large prostate >100g. 2- concomitant bladder pathology like stone or diverticulum, & 3- when dorsal lithotomy positioning is not possible. Its either transvesical or retropubic.
3-minimal invasiae therapy. 1- laser therapy, 2- electrovaporization of the prostate, 3- transurethral needle ablation, 4- high intensity focused ultrasound, 5- intraurethral stent, 6- balloon dilation of the prostate.