Download
1 / 34
530 likes | 1.14k Vues
HYPOTHYROIDISM. Edward Warren, MD, CMD, CAQ Geriatrics Chair, Geriatrics VCOM, Carolinas Campus May 6, 2012 12:45 pm. Goals. List causes of hypothyroidism. Diagnose hypothyroidism. Discuss clinical manifestations of hypothyroidism. Treat hypothyroidism. A natomy and Function.

E N D
HYPOTHYROIDISM Edward Warren, MD, CMD, CAQ Geriatrics Chair, Geriatrics VCOM, Carolinas Campus May 6, 2012 12:45 pm
Goals • List causes of hypothyroidism. • Diagnose hypothyroidism. • Discuss clinical manifestations of hypothyroidism. • Treat hypothyroidism.
Anatomy and Function • The thyroid gland is composed of follicles with fully iodinated thyroglobulin inside. • The follicular cells form the follicular walls. • Thyroid Releasing Hormone (TRH) from the hypothalamus stimulates elaboration of Thyroid Stimulating Hormone (TSH) by the pituitary. • TSH stimulates the absorption of thyroglobulin and secretion into the blood stream as T3 & T4. • The T3 and T4 provide negative feedback at the hypothalamus and pituitary.
Anatomy and Function • T4 is deiodinated to T3 in the thyroid and peripherally. • When T4 is deiodinated to form T3, some of it becomes an inactive form: Reverse T3. • The efficiency of this system with feedback loops allows TSH to be relied on to determine hypothyroidism (↑ TSH) and hyperthyroidism (↓ TSH).
Iodine • The thyroid extracts iodine from the serum with great efficiency. • A normal gland extracts 10 – 25% of radioactive iodine in tests. • In Graves’ disease (hyperthryroidism) it extracts 70 – 90%.
Iodine • Iodine deficiency is prevalent in the mountains of Africa, central South America, Europe, and northern Asia. • Iodine deficiency causes goiter and hypothyroidism.
Thyroid Serum Binding Proteins • Thyroid binding globulin carries 80% of the thyroid hormones. • Transthyretin (prealbumen) and albumen carry the rest. • Always measure free T3 and free T4 to get the unbound, functional levels.
T3 & T4 • T4 exceeds T3 20-fold when excreted. • Free T4 is 0.8 – 1.8 ng/l, is ⅓ as potent as T3, and has a half life of 7 days. • Free T3 is 2.0 – 5.0 pg/ml, 3 times as potent as T4, and has a half life of 18 hours.
Thyroid disorders are common in the elderly and are associated with significant morbidity if left untreated. Typical symptoms may be absent and may be erroneously attributed to normal aging or coexisting disease. Physical examination of the thyroid gland may not be helpful, as the gland is often shrunken and difficult to palpate. Hypothyroidism occurs in 10% of females and 2% of males in patients older than 60 years. Hypothyroidism
Risk Factors • Age over 60 years • Female gender • Goiter • Thyroid nodular disease • History of hypothyroidism, hyperthyroidism, thyroiditis • Family history of thyroid disease • History of radiotherapy for head and neck cancer • Nonthyroid autoimmune disease • Drugs (lithium, amiodarone)
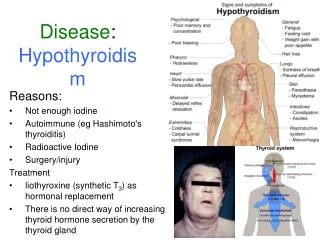
Causes Hashimoto's Thyroiditis Certain medications ¹³¹I therapy Radiation Surgical removal of thyroid Pituitary insufficiency (low TSH)
Symptoms (more frequent first) • Fatigue • Weakness • Dry, rough pale skin • Cold intolerance • Hair loss • Coarse, dry hair • Memory loss • Constipation • Weight gain with anorexia • Dyspnea • Hoarseness • Abnormal menstrual cycles • Hearing loss • Muscle cramps and myalgia • Depression • Irritability • Decreased libido
Signs (more frequent first) • Dry, coarse skin • Cool peripheral extremities • Puffy face, hands, & feet (myxedema) • Thin and brittle hair • Bradycardia, low BP, and low temperature • Edema • Delayed relaxation of reflexes • Pale, yellow skin • Loss of the outer edge of the eyebrows • Coarse facial features • Brittle nails • Mental slowing may be noted
Clinical manifestations Conditions associated with hypothyroidism: • Bilateral carpal tunnel syndrome • Urticaria (with autoimmune thyroid disease) • Pulmonary hypertension • Anemia (may be low Fe from heavy menses, or low B12) • Coagulopathy with easy bruising • Myopathy • Macrocytosis
Hashimoto's Thyroiditis • Hashimoto's Thyroiditis (autoimmune or chronic lymphocytic thyroiditis) is the most common cause of hypothyroidism. • It is named after the Japanese physician, Hakaru Hashimoto, who first described it in 1912. • During the course of this disease, the thyroid becomes inefficient in converting iodine into thyroid hormone and "compensates" by enlarging. • It occurs in 4/1000 women and 1/1000 men yearly.
Hashimoto's Thyroiditis • Thyroid antibodies are present in 95% of patients with Hashimoto's Thyroiditis and serve as a useful "marker" in identifying the disease without thyroid biopsy or surgery. • Thyroid antibodies may remain for years after the disease has been adequately treated and the patient is on thyroid hormone replacement. • The antibodies are usually directed against TPO (90%, prevent organification of I), thyroglobulin, or TSH receptors (blocking Ab, not stimulating as in Graves’). • It is clinically unnecessary to measure these antibodies in hypothyroidism.
Hashimoto's Thyroiditis • The radioactive iodine uptake may be paradoxically high in hypothyroidism because the gland retains the ability to "trap" iodine. • As the disease progresses, the TSH increases as the pituitary tries to induce the thyroid to make more hormone. There is a period of adequacy here with subclinical hypothyroidism. • The T4 eventually falls since the thyroid can't make it, and the patient becomes clinically hypothyroid. • This sequence of events occurs over a span of several weeks to months. • The thyroid gland is always enlarged, although only one side may be enlarged enough to feel. Treating with thyroid hormone replacement corrects the hypothyroidism and keeps the gland from enlarging more (it usually shrinks).
Drug Induced Hypothyroidism • Amiodarone: Decreased conversion of T4 to T3 (13% get hypothyroidism) • Dopamine: Acute decrease in TSH secretion • Lithium: Decreased thyroid hormone release and synthesis • Nitroprusside: Inhibits iodine trapping and thyroid hormone synthesis • Propylthiouracil, methimazole, para-aminosalicylic acid, 6-mercaptopurine, aminoglutethimide: Decreased thyroid hormone synthesis • Sulfonamides: Decreased thyroglobulin iodination and T4 synthesis • Iodine loading: • Jod-Basedow effect hyperthryroidism • Wolff-Chaikoff effect hypothyroidism
Amiodarone • Structurally similar to thyroid hormone • 39% iodine by weight • plasma iodine increases 40-fold and stays up for 6 months after stopping it • can induce hypothyroidism (Wolff-Chaikoff) • can induce hyperthyroidism (Jod-Basedow) especially in low iodine regions
Central (secondary) hypothyroidism Diseases that interfere with TRH production by the hypothalamus or that impair pituitary TSH production can produce central hypothyroidism. • Pituitary adenomas and associated surgery or radiotherapy • Tumors impinging on the hypothalamus or pituitary stalk • Traumatic transection of the pituitary stalk • Infiltrative diseases (e.g., sarcoidosis, hemochromatosis, and Langerhans cell histiocystosis) can interfere with hypothalamic TRH production or delivery. • Pituitary thyrotrope dysfunction can be caused by lymphocytic hypophysitis • Infection; metastatic disease; apoplexy (e.g., Sheehan syndrome or tumor infarction)
Diagnosis of Hypothyroidism • Confirmed by • elevated thyroid-stimulating hormone (TSH) level. • reduced free-T4 level • Subclinical hypothyroidism is diagnosed by • elevated TSH levels • normal free-T4 levels.
Antithyroid Antibodies: • The Most Clinically Important Ab are the • Antithyroid Microsomal Ab: called Anti-TPO • Thyroid Simulating Immunoglobulin. • The Anti-Thyroid PerOxidase Antibody • usually elevated in patients with Hashimoto’s Thyroiditis • may be used to help predict which patients with subclinical hypothyroidism (Normal Free T4 and elevated TSH) will go on to develop overt hypothyroidism.
Antithyroid Antibodies: • Thyroid Stimulating Immunoglobulins • associated with Grave’s Disease and are the likely cause of the hyperthyroidism seen in this condition. • These antibodies attach to the thyrotropin (TSH) receptor in the thyroid gland and activate it.
Other Laboratory Findings • increased cholesterol levels and dyslipidemia • increased liver enzymes • increased serum prolactin • low serum sodium • a complete blood count (CBC) that shows anemia
Myxedema Coma • Is a serious medical emergency that occurs when the body's level of thyroid hormones becomes extremely low. • It is treated with intravenous thyroid replacement and steroid therapy. • Supportive therapy of oxygen, assisted ventilation, fluid replacement, and intensive-care nursing may be indicated.
Treatment of Subclinical Hypothyroidism • A normal free-T4 with elevation of TSH values is found in subclinical hypothyroidism. • The point at which therapy should be initiated has been controversial. • The work-up for this condition should include anti-TPO antibodies • Patients with positive tests for thyroid antibodies should be treated. • Patients whose tests for thyroid antibodies are negative, but whose TSH values are >10 mg/mL, should also be treated. • Patients with goiter, elevated lipid levels, pregnancy, ovulatory dysfunction/infertility, or impaired cardiac contractility may also be treated.
Treatment • Hypothyroidism is treated with levothyroxine. • The dose of levothyroxine required in adults is about 1.0 to 1.7 µg/kg. • Start the elderly and those with weak hearts on just 25 mcg levothyroxine daily. Otherwise it precipitates heart failure. • There is no hurry since the smallest dose prevents all complications and ends symptoms.
Treatment • It is titrated against the TSH level, which should be lowered to about the midpoint of the normal range. • The patient should be seen back in approximately 2 months, the period that it takes for the TSH to reach steady state. • Once thyroid function tests and clinical status are stable, thyroid function tests should be monitored approximately every 6 to 12 months.
Hyperthyroidism in Brief • Generally caused by Graves’ Disease with antibodies against TSH receptors that also activate them. • It can be from hyperactive nodules. • The TSH is low and the T4 or T3 are high. • Treatment is to ablate the thyroid with radiation from ¹³¹I, surgically remove it, or suppress it with medication (propylthiouracil or methimazole).
Euthyroid Sick Syndrome • In the setting of acute, severe illnesses, or malnutrition, the TSH and T4 are normal, but the T3 is low. • Recognize this to avoid unnecessary treatment. • Avoid doing thyroid studies in ill, debilitated people.
References • http://www.medscape.com/viewarticle/433851