Download
1 / 86
1k likes | 2.4k Vues
Acute Gastroenteritis. Dr Mohamed Abu nada Pediatric neurology department Dr. Al Rantisi Specialized children hospital. ETIOLOGY AND EPIDEMIOLOGY. Acute enteritis or acute gastroenteritis refers to diarrhea , which is abnormal frequency and liquidity of fecal discharges.

E N D
Acute Gastroenteritis Dr Mohamed Abu nada Pediatric neurology department Dr. Al Rantisi Specialized children hospital
ETIOLOGY AND EPIDEMIOLOGY • Acute enteritis or acute gastroenteritis refers to diarrhea, which is abnormal frequency and liquidity of fecal discharges. • Diarrhea is caused by many different infectious or inflammatory processes in the intestine • These processes directly affect enterocyte secretory and absorptive functions • Enteritis has many viral, bacterial, and parasitic causes
Diarrhea is the leading cause of morbidity and the second most common disease in children in the U.S. • In the developing world, it is a major cause of childhood mortality. • The epidemiology of gastroenteritis depends on the specific organisms. • Some organisms are spread person to person, others are spread via contaminated food or water, and some are spread from animal to human. Many organisms spread by multiple routes. • The ability of an organism to infect relates to its mode of spread, its ability to colonize the gastrointestinal tract, and the number of organisms required to cause disease.
Viral causes • rotaviruses, caliciviruses, astroviruses, and enteric adenoviruses (serotypes 40 and 41). • Rotavirus invades the epithelium and damages villi of the upper small intestine and in severe cases involves the entire small bowel and colon. Rotavirus is the most frequent cause of diarrhea during the winter months
Typhoid fever • caused by Salmonella typhi and occasionally Salmonella paratyphi. • These infections are distinguished by their potential for prolonged fever, inconsistent presence of diarrhea, and extraintestinal manifestations. • Worldwide there are an estimated 16 million cases of typhoid fever annually, resulting in 600,000 deaths.
Nontyphoidal Salmonella • produce diarrhea by invading the intestinal mucosa. The organisms are transmitted through contact with infected animals (chickens, turtles) or from contaminated food products, such as dairy products, eggs, and poultry. • Infected persons without symptoms, or chronic carriers, serve as reservoirs and sources of continuous spread. Carriers often have cholelithiasis. • The incubation period for gastroenteritis ranges from 6 to 72 hours, but usually is less than 24 hours.
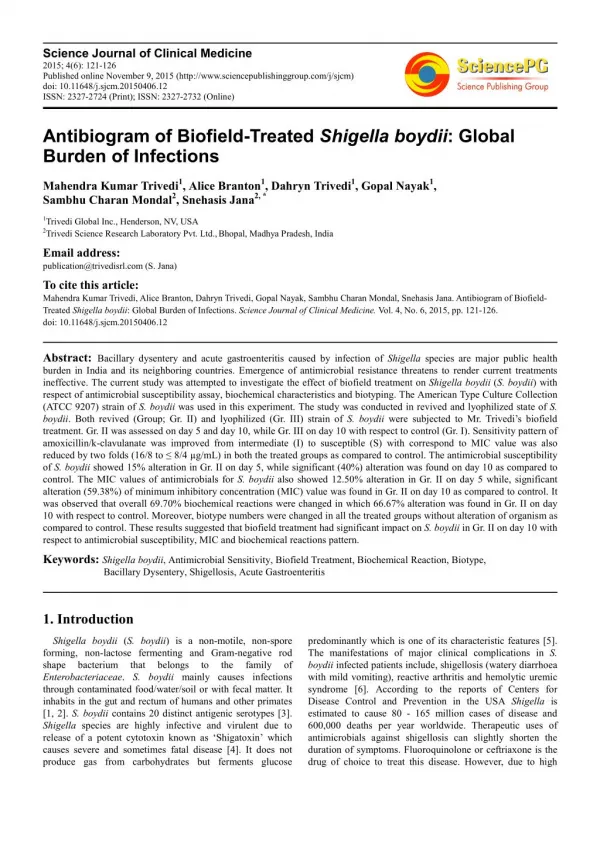
Shigella dysenteriae • disease by producing Shiga toxin, either alone or combined with tissue invasion. • The incubation period is 1 to 7 days • Infection is spread by person-to-person contact or by the ingestion of contaminated food with 10 to 100 organisms. • The colon is selectively affected. • High fever and seizures may occur, in addition to diarrhea.
E. coli • Only certain strains of E. coli produce diarrhea. • E. coli strains associated with enteritis are classified by the mechanism of diarrhea: 1.enteropathogenic (EPEC), 2.enterotoxigenic (ETEC), 3.enteroinvasive (EIEC), 4.entero-hemorrhagic (EHEC), or 5.enteroaggregative (EAEC). EPEC is responsible for many of the epidemics of diarrhea in newborn nurseries and in daycare centers. ETEC produce heat-labile (cholera-like) enterotoxin, heat-stable enterotoxin, or both. causes 40% to 60% of cases of traveler's diarrhea.
E. Coli cont. • EHEC is associated with contaminated food, including unpasteurized fruit juices and especially undercooked beef. EHEC is associated with a self-limited form of gastroenteritis, usually with bloody diarrhea, • EIEC invades the colonic mucosa, producing widespread mucosal damage with acute inflammation, similar to Shigella. EHEC, especially the E. coli O157:H7 strain, produce a Shiga-like toxin that is responsible for a hemorrhagic colitis and most cases of hemolytic uremic syndrome (HUS)
Campylobacter jejuni • accounts for 15% of bacterial diarrhea. • The infection is spread by person-to-person contact and by contaminated water and food, especially poultry, raw milk, and cheese. • The organism invades the mucosa of the jejunum, ileum, and colon, producing enterocolitis.
Yersinia enterocolitica • is transmitted by pets and contaminated food, especially chitterlings. • Infants and young children diarrhea • Older children acute lesions of the terminal ileum or acute mesenteric lymphadenitis mimicking appendicitis or Crohn disease. • Arthritis, rash, and spondylopathy may develop.
Clostridium difficile • causes C. difficile-associated diarrhea, or antibiotic-associated diarrhea secondary to its toxin. • The organism produces spores that spread from person to person. • C. difficile-associated diarrhea may follow exposure to any antibiotics, but is classically associated with clindamycin.
Entamoeba histolytica (amebiasis), Giardia lamblia • E. histolytica infects the colon; amebae may pass through the bowel wall and invade the liver, lung, and brain. Diarrhea is of acute onset, is bloody, and contains WBCs. • G. lamblia is transmitted through ingestion of cysts, either from contact with an infected individual or from food or freshwater or well water contaminated with infected feces.
CLINICAL MANIFESTATIONS • fever, lethargy, and abdominal pain. • Viral diarrhea watery stools, with no blood or mucus. Vomiting may be present, and dehydration may be prominent. Fever, when present, is low grade. • Typhoid fever, caused by S. typhi and S. paratyphi, is characterized by bacteremia and fever. There is fever, headache, and abdominal pain that worsen over 48 to 72 hours with nausea, decreased appetite, and constipation over the first week. • Dysentery is diarrhea with blood and mucus, possibly foul smelling, and fever. • Insidious onset of progressive anorexia, nausea, gaseousness, abdominal distention, watery diarrhea, secondary lactose intolerance, and weight loss is characteristic of giardiasis.
Dehydration • assess the degree of dehydration • Mild dehydration (3% to 5%) is characterized by normal pulse rate or minimal tachycardia, decreased urine output, thirst, and normal P/E. • Moderate dehydration (5% to 10%) - tachycardia, - little or no urine output, - irritability or lethargy, - sunken eyes and fontanel, - decreased tears, - dry mucous membranes, - mild tenting of the skin, and - delayed capillary refill (≤ 2 seconds) .
Severe dehydration (10% to 15%) - tachycardia with a weak pulse - hypotension - no urine output - extremely sunken eyes and fontanel - no tears - parched mucous membranes - tenting of the skin - extremely delayed capillary refill (≥ 3 seconds) with cold and mottled skin.
Mild to moderate dehydration usually can be treated with oral rehydration, • severe dehydration usually requires IV rehydration. Severe dehydration may require ICU admission.
LABORATORY AND IMAGING STUDIES • CBC, electrolytes, BUN, creatinine. • Stool specimens should be examined for mucus, blood, and leukocytes, which indicate colitis • A positive fecal leukocyte examination indicates the presence of an invasive or cytotoxin-producing organism, such as Shigella, Salmonella, C. jejuni, and invasive E. coli. • Patients infected with Shiga toxin-producing E. coli and E. histolytica generally have minimal fecal leukocytes.
LABORATORY AND IMAGING STUDIES (cont.) • A rapid diagnostic test for rotavirus in stool should be performed. • Stool cultures are recommended for patients with fever, profuse diarrhea, and dehydration or if HUS is suspected. • If the stool test result is negative for blood and WBCs, and there is no history to suggest contaminated food ingestion, a viral etiology is most likely.
LABORATORY AND IMAGING STUDIES (cont) • Stool evaluation for parasitic agents. • Positive blood cultures are uncommon with bacterial enteritis except for S. typhi (typhoid fever) and for nontyphoidal Salmonella and E. coli enteritis in very young infants.
LABORATORY AND IMAGING STUDIES (cont) • In typhoid fever, blood cultures are positive early in the disease, whereas stool cultures become positive only after the secondary bacteremia • The diagnosis of E. histolytica is based on identification of the organism in the stool. Serologic tests are useful for diagnosis of extraintestinal amebiasis, including amebic hepatic abscess. • Giardiasis can be diagnosed by identifying trophozoites or cysts in stool
TREATMENT • Most infectious causes of diarrhea in children are self-limited. • Management of viral and most bacterial causes of diarrhea is primarily supportive and consists of correcting dehydration and ongoing fluid and electrolyte deficits and managing secondary complications resulting from mucosal injury. • Antibiotic treatment is recommended for only some bacterial and parasitic causes of diarrhea
Treatment of Salmonella • Antibiotic treatment of mild illness with Salmonella does not shorten the clinical course, but does prolong bacterial excretion. • Antibiotic therapy is necessary only for patients with S. typhi (typhoid fever) and sepsis or bacteremia with signs of systemic toxicity, or age < 3 months with nontyphoidal salmonella.
Treatment of shigella • Antibiotic treatment of Shigella produces a bacteriologic cure in 80% of patients after 48 hours, reducing the spread of the disease. • Many Shigella sonnei isolates, the predominant strain affecting children, are resistant to amoxicillin and TMP-SMZ. • Recommended treatment for children is an oral third-generation cephalosporin (cefixime, cefpodoxime)or iv ceftriaxone, .
Treatment of E. Coli • Antibiotic treatment of E. coli enteritis is indicated for infants younger than 3 months old with EPEC and patients who remain symptomatic. • Antibiotic treatment is not recommended for patients with E. coli O157:H7 or HUS because release of toxin may precipitate or worsen the course of HUS.
Treatment of Campylobacter • Most patients with Campylobacter recover spontaneously before the diagnosis is established. • Treatment with erythromycin, azithromycin, initiated within 5 days of the onset of illness speeds recovery and reduces the duration of the carrier state.
Treatment of C. difficile • Treatment of C. difficile includes discontinuation of the AB and, if diarrhea is severe, oral metronidazole or Vancomycin.
E. histolytica dysentery is treated with metronidazole followed by a luminal agent, such as iodoquinol. • The treatment of G. lamblia is with albendazole, metronidazole, furazolidone. • Drugs such as loperamide, and diphenoxylate are potentially dangerous and have no place in the management of acute infectious diarrhea in children
COMPLICATIONS • The major complication of GE is dehydration and the cardiovascular compromise that can occur with severe hypovolemia. • Intestinal abscesses ( Shigella and Salmonella infections, especially typhoid fever) leading to intestinal perforation. • Severe vomiting associated with GE can cause esophageal tears or aspiration.
PREVENTION • clean, uncontaminated water and proper hygiene in growing, collecting, and preparing foods. • Good hygienic measures, especially good hand washing with soap and water • poultry products, such as eggs, should be considered potentially contaminated with Salmonella and should be handled and cooked appropriately. • Recommendations for travelers are for presumptive self-treatment for 3 days with TMP-SMZ for children which are initiated at the first signs of diarrhea, nausea, bloating, or urgency. • Lactobacillus acidophilus has been recommended as a probiotic to prevent antibiotic-associated diarrhea
Degrees of dehydration • Mild dehydration (3 – 5 % weight loss, 30 – 50 ml/Kg). • Moderate dehydration (6 – 9 % weight loss, 60 – 90 ml/Kg). • Severe dehydration (10 % or more, 100 ml/Kg or more).
Types of dehydration • Hyponatremic dehydration (Na+ < 130 mEq/L). • Isonatremic dehydration (Na+ 130 – 150 mEq/L). • Hypernatremic dehydration (Na+ > 150 mEq/L).
Phases of therapy • Mild to moderate dehydration is replaced with 150 ml/Kg/day oral rehydration solution (ORS). • Treatment with ORS is simple and enables management of uncomplicated cases at home, regardless of etiologic agent. • Early administration of ORS leads to fewer office, clinic, and ED visits and to potentially fewer hospitalizations and deaths.
Moderate to severe dehydration is managed in the hospital with IV fluid. Therapy is divided into three phases: • Initial therapy: aim to restore IVF to improve circulatory and renal functions. • Subsequent therapy: aim to replace deficit, supply maintenance, and replace ongoing losses. • Final phase: aims to restore normal intake output balance.
Principles of therapy • In all form of dehydration: shock, acidosis, and hypoglycemia are treated aggressively, but rehydration should be more controlled. • Isonatremic dehydration is corrected over one day. • Hyponatremic dehydration is corrected over two days. • Hypernatremic dehydration is corrected over 2 – 3 days.
SEVERE DEHYDRATIONInitial therapy volume expanders (crystalloids and / ± colloid) are initially indicated in all types of severe dehydration • Normal Saline (NS) is preferred where shock is associated with metabolic alkalosis, risk of increase intracranial pressure and hyperosmolar states. • Ringer Lactate (RL) is preferred where shock is associated with metabolic acidosis.
SUBSEQUENT THERAPYIsonatremic dehydration • Fluid deficit: 150 ml/Kg minus initial therapy. • Na+ deficit: 7 – 10 mEq/Kg minus initial therapy. • Fluid: Half as D5% S0.45% over 8 hours. • Half as D5% S0.18% over 16 hours. • Maintenance: no modification. • Ongoing loss: calculate volume, determine type and replace over suitable time.
Application 10 Kg infant with severe isonatremic dehydration • Initial therapy: 20 ml/Kg (200 ml NS contain 30 mEq Na+) repeat once or twice. • Fluid deficit: 150 ml/Kg minus initial therapy = 1500 – 200 = 1300 ml. • Na+ deficit: 10 mEq/Kg minus initial therapy = 100 – 30 = 70 mEq. • Half deficit (8 h): = 750 – 200 = 550 ml D5% S0.45% contain 40 mEq of Na+. • Half deficit (16 h): = 750 ml D4.3% S0.18% contain 25 mEq of Na+. • Maintenance (24 h): = 100 ml/Kg = 1000 ml D4.3% S0.18% contain 31 mEq of Na+.
Hyponatremic dehydration • Fluid deficit: 75 ml/Kg minus initial therapy. • Na+ deficit: 10 – 15 mEq/Kg minus initial therapy. • Fluid deficit: • Asymptomatic hyponatremia: NS over one to two days. • Symptomatic hyponatremia: 3 % saline, 12 ml/Kg at a rate of one ml/minute, then as asymptomatic hyponatremia. • Maintenance: No modification. • Ongoing loss: Calculate volume, determine type, and replace over suitable time.
Application10 Kg infant with severe asymptomatic hyponatremic dehydration (Na+ = 125) • Initial therapy: 20 ml/Kg (200 ml of NS contain 30 mEq. Na+). • Fluid deficit: 75 ml/Kg – initial therapy = 750 - 200 = 550 ml. • Na+ deficit: 10 mEq/Kg – initial therapy = 100 – 30 = 70 mEq. • Plan: 550 ml of NS contain 80 mEq of Na+ are given over 1 – 2 days. • Maintenance: 100 ml/Kg = 1000 ml D4.3% S0.18 contains 31 mEq of Na+.
Application10 Kg infant with severe symptomatic hyponatremic dehydration (Na+ = 113) • Initial therapy: 20 ml/Kg (200 ml of NS contain 30 mEq. Na+). • Fluid deficit: 75 ml/Kg – initial therapy = 750 - 200 = 550 ml. • Na+ deficit: 15 mEq/Kg – initial therapy = 150 – 30 = 120 mEq. • Plan: - 12 ml/Kg of 3 % hypertonic saline = 120 ml over 2 hours (1 ml/min) Contain 60 mEq Na+. - 550 ml of NS contain 80 mEq of Na+ are given over 1 – 2 days. • Maintenance: 100 ml/Kg = 1000 ml D4.3% S0.18 contains 31 mEq of Na
Hypernatremic dehydration • Fluid deficit: 125 ml/Kg minus initial therapy. • Na+ deficit: 2 – 5 mEq/Kg minus initial therapy. • Fluid deficit: - D4.3% S0.18 over 2 to 3 days. - If convulsions occur during treatment use 3 – 5 ml/Kg of 3 % hypertonic saline at 1 ml/min infusion rate. • Maintenance: 70 % of maintenance is given. • Ongoing loss: Calculate volume, determine type, and replace over suitable time.
Application10 Kg infant with severe hypernatremic dehydration (Na+ >150) • Initial therapy: 20 ml/Kg (200 ml of NS contain 30 mEq. Na+). • Fluid deficit: 125 ml/Kg – initial therapy = 1250 - 200 = 1050 ml. • Na+ deficit: 5 mEq/Kg – initial therapy = 50 – 30 = 20 mEq. • Plan: 1250 ml of D4.3% S0.18 contain 40 mEq of Na+ are given over 2 – 3days. • Maintenance: 70 ml/Kg = 700 ml D4.3% S0.18 contains 20 mEq of Na+.
Application 10 Kg infant with severe hypernatremic dehydration (Na+ >150) • Day 1: 70 ml maintenance + 50 ml deficit = 120 ml/Kg = 1200 ml (Na+ 36 mEq). • Day 2: 70 ml maintenance + 50 ml deficit = 120 ml/Kg = 1200 ml (Na+ 36 mEq). • Day 3: 70 ml maintenance + 25 ml deficit = 95 ml/Kg = 950 ml (Na+ 30 mEq).
POTASSIUM THERAPY • Normal blood potassium level: • Less than 2 months: 3 – 7 mEq/L. • 2 – 12 months: 3.5 – 6 mEq/L. • More than 12 months: 3.5 – 5 mEq/L. • Normal daily requirements: 2 – 3 mEq/Kg/day.
HYPOKALEMIA (serum K+ < 3 mEq/L) • Hypokalemia is usually not a real emergency. • Extremely acute severe hypokalemia may lead to death through cardiac arrhythmia or respiratory muscle paralysis.
Treatment of hypokalemia • Oral potassium therapy:For chronic hypokalemia as in diarrheal disorders. Oral K+ salts are given in a dose 2- 4 mEq/Kg/day. Doses as high as 15 mEq/Kg/day may be needed.
Intravenous potassium therapy • Calculate K+ deficit: K+ deficit = (3 – current K+) X 0.3 X body weight • Replace according to following rules: • Don’t exceed 40 mEq/L conc. via peripheral line. • Don’t exceed 80 mEq/L conc. via central line. • Don’t exceed 0.3 mEq/Kg/hour infusion rate. • For life threatening hypokalemia give 1 mEq/Kg/hour via central line under continuous ECG monitoring. • Stop this infusion as soon as life threatening hypokalemia disappears.