Download
1 / 29
301 likes | 620 Vues
Higher Human Biology . Unit 1: Cell Function and Inheritance. Chapter 14: Genetic Screening and Counselling. Learning Intentions. By the end of this lesson you should be able to- describe Genetic screening and counselling . Explain the use of family histories in determining genotypes.

E N D
Higher Human Biology Unit 1: Cell Function and Inheritance Chapter 14: Genetic Screening and Counselling. Mrs Smith: Ch14: Genetic Screening and Councilling
Learning Intentions • By the end of this lesson you should be able to- • describe Genetic screening and counselling. • Explain the use of family histories in determining genotypes. • Examples might include albinism, Huntington’s chorea, cystic fibrosis, phenylketonuria, haemophilia and muscular dystrophy. • Explain the use of karyotypes of foetal material where there is a possibility of genetic disorder. • Discuss risk evaluation in cases of polygenic inheritance. • Understand post-natal screening for conditions which have a genetic basis. Mrs Smith: Ch13: Mutations an Chromosomal Abnormalities
You need to know these words PKU Klinefelter’s Syndrome Genetic Screening Councilling Pedigree Autosomal dominant Inheritance Haemophilia Sex-linked recessive trait Prenatal Autosomal Recessive inheritance Post-natal Cystic fibrosis Chorionic villus sampling Huntingtons Chorea Mrs Smith: Ch13: Mutations an Chromosomal Abnormalities Risk Evaluation Amniocentesis
Use of Family Histories • A pattern of human inheritance can be revealed by collecting information about a particular characteristic from the members of a family and then using it to construct a family tree (pedigree) Mrs Smith: Ch14: Genetic Screening and Councilling
Types of pedigree • There are 3 types of pedigree that you need to know about • Autosomal recessive inheritance • Autosomal dominant inheritance • Sex-linked recessive trait. Mrs Smith: Ch14: Genetic Screening and Councilling
The Geneticist recognises Autosomal Recessive Inheritance because.... • The trait is rarely expressed • The trait tends to skip generations • The trait is expressed in some cousins • Males and females are equally affected • All sufferers of the trait are homozygous recessive • Non-sufferers are homozygous dominant or heterozygous. Mrs Smith: Ch14: Genetic Screening and Councilling
Autosomal recessive inheritancee.g Cystic Fibrosis Mrs Smith: Ch14: Genetic Screening and Councilling
The Geneticist recognises Autosomal Dominant Inheritance because.... • The trait appears in every generation. • Each sufferer has an affected parent. • When a branch of the family does not express the trait it fails to reappear in future generations of that branch. • Males and females are equally affected. • All non-sufferers are homozygous. • Sufferers are homozygous dominant or heterozygous. Mrs Smith: Ch14: Genetic Screening and Councilling
Autosomal Dominant Inheritancee.g. Huntington’s Chorea Mrs Smith: Ch14: Genetic Screening and Councilling
The Geneticist recognises Sex-linked recessive because..... • More males are affected than females • None of the sons of an affected male show the trait • Some grandsons of affected males show the trait • All sufferers of the trait are homozygous recessive • Non-sufferers are homozygous dominantor or heterozygous carrier females Mrs Smith: Ch14: Genetic Screening and Councilling
Sex-linked recessive traite.g. haemophilia Mrs Smith: Ch14: Genetic Screening and Councilling
Sex-linked recessive traite.g. haemophilia Mrs Smith: Ch14: Genetic Screening and Councilling
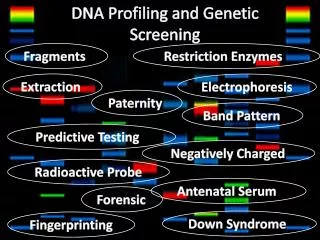
FYI - Genetic code • In 1966, the Genetic code was discovered • Human Genome Project to determine nucleotide sequence of human DNA began in 1990 and was completed in 2003. • Scientists are now able to predict characteristics by studying DNA. This leads to genetic engineering, genetic counseling. Mrs Smith: Ch14: Genetic Screening and Councilling
Genetic code An international team of scientists began the project to map the human genome. Mrs Smith: Ch14: Genetic Screening and Councilling
Genetic Code Mrs Smith: Ch14: Genetic Screening and Councilling
Genetic Code In 1990, gene therapy was used on patients for the first time Mrs Smith: Ch14: Genetic Screening and Councilling
Assessing the risk! • Once the genetic councillor has constructed the family tree(s) and established as many genotypes as possible, he/she is in a position to assess the risk and state the possibilities. Mrs Smith: Ch14: Genetic Screening and Councilling
Assessing the risk – Autosomal recessive. e.g. cystic fibrosis • If a couple were considering having a family, however the female knows cystic fibrosis runs in her family but not in her partners. • They could approach a genetic councillor. • By analysing her family tree the councillor could work out there was a 2:3 chance that the female is a carrier. • The councillor would already know the frequency in the British population as 1:25 for carrying the heterozygous allele for CF – this is the risk of her partner being a carrier. • The councillor would then conclude the risk of having a child with CF as low. Mrs Smith: Ch14: Genetic Screening and Councilling
Assessing the risk – Autosomal Dominant. e.g. Huntington’s chorea • Consider a brother and sister, unlike their siblings they are too young to know if they have received the harmful allele from an affected parent. • They could approach a genetic councillor. • The councillor would already know the frequency in the British population, and there is a 1:2 chance that each is heterozygous allele for HC • By analysing her family tree the councillor would then conclude the risk of having of each sibling suffering this debilitating disease as high. Mrs Smith: Ch14: Genetic Screening and Councilling
Assessing the risk – sex-linked. e.g. Haemophilia • If a couple were considering having a family, however the female knows Haemophilia runs in her family but not in her partners. She is anxious to know if she could pass the trait onto her sons. • They could approach a genetic councillor. • By analysing her family tree the councillor would note that the woman's brother and sisters son her nephew have developed this sex linked trait. • This shows her sister and mother are carriers. • The councillor would then conclude a she has a 1:2 risk of being carrier and a 1:4 risk that each son will be a haemophiliac. Mrs Smith: Ch14: Genetic Screening and Councilling
Advantage and disadvantagr of Genetic counselling • The aim of genetic counselling is to help people to make well informed decisions for themselves based on information available. • Advantage: Analysis of a family tree allows the expert to chart he pattern of the disorder. • Disadvantage: It is of limited value in that it can only offer an assessment of risk. Mrs Smith: Ch14: Genetic Screening and Councilling
Pre-natal Screening • If after assessing the risk of having baby with a genetic disorder. AND IF the couple decide to go ahead and have a baby pre-natal screening can be employed. • Two methods of pre-natal screening depend on foetal material being obtained to allow karyotypes to be examined • Amniocentesis • Chorionic villus sampling (CVS) Mrs Smith: Ch14: Genetic Screening and Councilling
Amniocentesis • Amniocentesis is carried out in the 18th week of pregnancy. • It involves the withdrawal of a little amniotic fluid containing foetal cells. • These cells can be analysed and a full karotype made. • It slightly increases risk of miscarriage
Chorionic Villus Sampling • A small tube is inserted into the womans reproductive tract, placental cells are removed, these cells are used for karyotyping • ADV: CVS can be carried out at 8 weeks of pregnancy • DISADV: Causes a higher risk of miscarriage then amniocentesis
Post-natal Screening • At present none of the inherited disorders can be successfully treated except for PKU • Phenylketonuria results from an inborn error of metabolism for 1:10000 b irths in Britain. • If not detected soon after birth the baby suffers from mental retardation • All British babies are routinely tested for excess phenylalanine after birth by means of a blood test Mrs Smith: Ch14: Genetic Screening and Councilling
Testing for PKU: Guthrie's test Mrs Smith: Ch14: Genetic Screening and Councilling
Task: TYK -Torrance pg106 Qu’s 1-3 Mrs Smith: Ch13: Mutations an Chromosomal Abnormalities
Task: AYK -Torrance pg 106-7 Qu’s 1-4 Applying your knowledge Mrs Smith: Ch13: Mutations an Chromosomal Abnormalities
Essay Question Guide to H-Grade essays pg 64 By means o examples you have studied discuss genetic conditions of medical importance with reference to the following: • Family History • Use of Karyotypes • Post-natal Screening. (15) Mrs Smith