Download
1 / 35
350 likes | 473 Vues
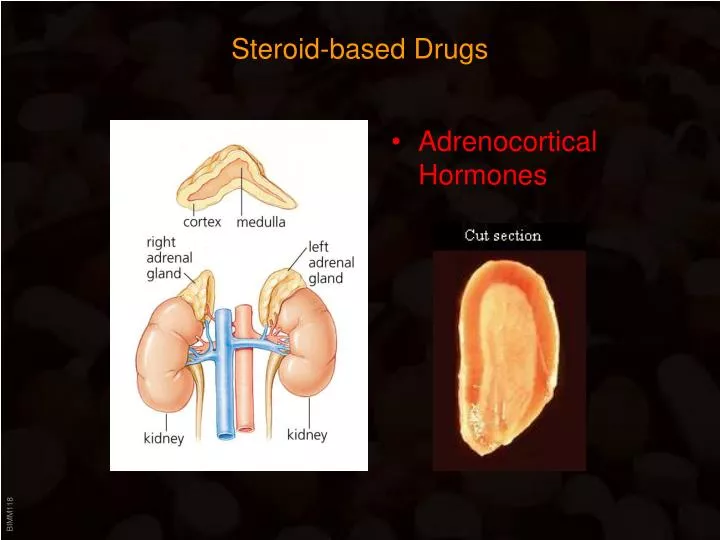
Steroid-based Drugs. Adrenocortical Hormones. Adrenocortical Hormones. Adrenal gland : Medulla : produces Epinephrine (stimulated by sympathetic impulse) Cortex : Zona glomerulosa – produces Aldosterone (stimulated by Angiotensin II and ACTH)

E N D
Steroid-based Drugs • Adrenocortical Hormones
Adrenocortical Hormones Adrenal gland: • Medulla: • produces Epinephrine(stimulated by sympathetic impulse) • Cortex: • Zona glomerulosa – produces Aldosterone(stimulated by Angiotensin II and ACTH) • Zona fasciculata – produces Glucocorticoids(stimulated by ACTH = Corticotropin) • Zona reticularis – produces Androgens(physiological role unclear)
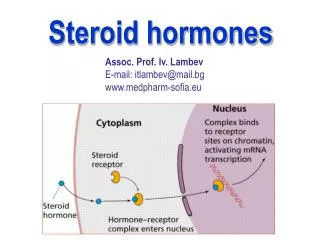
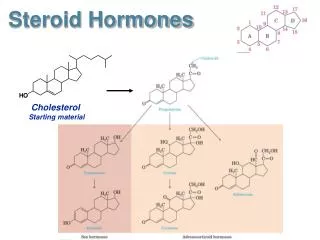
Adrenocortical Hormones Steroid hormone synthesis: • Pregnenolone synthesis is rate-limiting step • C21 hydroxylase: • Prevents hydroxylation of C17 (-> c) => Only mineralocorticoids • C17 hydroxylase: • Hydroxylation of C17 (-> f, g) can be followed by hydroxylation of C11 and C21 (-> h, j, k) => Sex hormones and glucocorticoids • P450C17a hydroxylase: • Produces 17-Keto-steroids (-> l) => Sex hormones
Adrenocortical Hormones Steroid hormone classification: • Progesterone: • C21 • C 3: =O • C17: -OH or =O • Mineralocorticoids: • C21 • C21: -OH • C3: =O • Glucocorticoids : • C21 • C21, C17: -OH • C 3: =O • C11: -OH or =O • Estrogens : • C18 • C17: -OH or =O • C 3: -OH • Androgens : • C19 • C17: -OH • C 3: =O
Adrenocortical Hormones Glucocorticoids (GC): • Inhibit all phases of inflammatory reaction • Promote fetal development (lungs) • Inhibit NFkB nuclear translocation => transcription of proinflammatory mediators is prevented • Upregulate lipocortin => inhibits PLA2 => no PG and LT synthesis • Undesirable effects of increased GC: • Immune suppression • Increased glucose release (=> “steroid diabetes”) • Glucose coverted to fat => adiposity • Increased protein catabolism => muscle atrophy • Salt and water retention (increased GC lead to reduction in ACTH => decreases levels of aldosterone) => hypertension • Osteoporosis
Adrenocortical Hormones Glucocorticoids (GC): • Adrenal cortex failure (= Addison’s disease) Lack of GC production: • Chronic fatigue and muscle weakness. • Loss of appetite, inability to digest food, and weight loss. • Low blood pressure (hypotension) • Blotchy, dark tanning and freckling of the skin (feedback missing => increased corticotropin) • Blood sugar abnormalities • Inability to cope with stress • Adrenal cortex tumors (= Cushing Syndrome) GC overproduction • Upper body obesity • “Buffalo hump” • Red, round face • Hypertension • Water retention • Thin skin and bruising • Poor wound healing
Adrenocortical Hormones Glucocorticoids (GC): Clinical uses: • Allergic Rhinitis • Rheumatoid Arthritis • Asthma • Multiple Sclerosis • Carpal Tunnel Syndrome • Dermatitis • COPD • Osteoarthritis • Gout • Psoriasis • Inflammatory Bowel Disease • Sinusitis • Lupus Erythematosus • Many conditions flare up if GC therapy is discontinued due to adreno-corticol atrophy
Adrenocortical Hormones Glucocorticoids (GC): • Hydrocortison (= Cortisol) • Main glucocortocoid in humans • Also binds mineralocorticoid receptor (Cortison does NOT) • Used for replacement therapy (Addison’s Disease) • Otherwise mostly topical application due tosodium-retaining effects
Prednisone Prednisolone Adrenocortical Hormones Glucocorticoids (GC): • Prednisone • Inactive until converted to • Prednisolone • Drug of choice for systemic application • Lower sodium-retaining effects
Adrenocortical Hormones Glucocorticoids (GC): • Triamcinoline • Stronger anti-inflammatory (5x) than cortisol • No sodium-retaining effect HalogenatedGC • Betamethasone • Dexamethasone • 30x more potent than cortisol • No water and sodium retaining effects
Adrenocortical Hormones Glucocorticoids (GC): • Administration • Oral • Nasal • Cutaneous • IV • Inhalation
Steroid-based Drugs • Sex Steroids
Sex Steroids • Female reproductive cycle • Gonadotropin Releasing Hormone(GnRH) = Gonadoliberin stimulates release of • Follicle stimulating hormone(FSH) = Follitropin and • Luteinising Hormone(LH) = Lutropin which trigger production of • Estrogens (E) and Gestagens (G) which in turn negatively regulate • Pituitary (E+G) and Hypothalamus (G)hormone production
Sex Steroids • Female reproductive cycle • Cycle length varies from 21-35 days • Menstruation 3-6 days • First (= Proliferative) phase: • Variable (7-21 days) • FSH and LH promote follicle development • One follicle becomes the Graafian follicle(the rest degenerate) • Graaffian Follicle: • Consists of thecal and granulosa cellswhich surround the ovum • FSH-stimulated granulosa cells produce estrogens from androgen precursors generated by LH-stimulated thecal cells • Estrogens are responsible for the proliferative phase: increase in thickness and vascularity of endometrium; secretion of protein+ carbo-rich mucus • Constant low estrogen inhibits LH/FSH production BUT high estrogen cause surge of LH production => swelling and rupture of Graafian follicle = Ovulation
Sex Steroids • Female reproductive cycle • Second (= Secretory) phase: • Secretory phase constant (~ 14 days) • LH-stimulated ruptured follicle developsinto Corpus luteum which secretsProgesterone • Progesterone (Pg) is responsible for the secretory phase: endometrium becomessuitable for implantation; mucus thickens • Thermogenic effects of Pg =>body temperature increase 0.5º C • Without implantation: Pg secretion stops=> menstruation is triggered • With implantation: continued Pg productionwhich (via inhibition of LH and FSH prod.) blocks further ovulation • Chorion (“precursor” of placenta) secreteshuman chorionic gonadotropin (HCG) whichmaintains endometrium lining throughoutpregnancy (HCG -> see pregnancy test)
Sex Steroids • Female reproductive cycle
Sex Steroids Estrogens All produced from androgen precursors Three main endogenous estrogens: • Estradiol • Primary estrogen in humans • Breast development • Improving bone density • Growth of the uterus • Accelerating bone maturation and epiphyses closure • Development of the endometrium to support pregnancy • Promoting vaginal mucosal thickness and secretions • Increase HDL • Estrone • Estriol • only during pregnancy (made by fetus)
Sex Steroids Estrogens • Estrogensinduce expression of progesterone receptors • Progesteroneinhibits expression of estrogen receptors • Two types of estrogen receptors => potential for selective drugs • Estradiol • Not suitable for oral administration (rapid hepatic elimination) => stable derivatives: • Ethinylestradiol • Diethyl-Stilbestrol • Stilbene derivative
Sex Steroids Estrogens • Mestranol • Used in oral contraceptives • Inactive => Cleavage of C3-methoxy group yields ethinylestradiol • Raloxifene • Selective estrogen receptor modifier (=SERM) • Antiestrogenic effects on breast and endometrium • Estrogenic effects on bone and lipid metabolism => use in postmenopausal osteoporosis Clinical uses of estrogens: • Replacement therapy (Turner syndrome; menopause) • Contraception • Cancer therapy
Sex Steroids Anti-Estrogens • Tamoxifen • Antiestrogenic effects on mammary tissue • Weak estrogenic effects on bone and lipid metabolism • Clomiphene • Inhibits estrogen binding in the pituitary=> prevention of negative feedback=> ovulation Clinical uses of anti-estrogens: • Breast cancer therapy (Tamoxifen) • Infertility (Clomiphen)
Sex Steroids Progesterons • Progesterone • Inhibits rhythmic contractions of the myometrium • Not suitable for oral administration (rapid hepatic elimination) => stable derivatives: • Hydroxyprogesterone • Medroxyprogesterone
Sex Steroids Progesterons Testosterone derivatives with progesterone activity: • Norethindrone • Norgestrel • Desogestrel
Sex Steroids Anti-Progesterons • Mifepristone (RU486) • developed during the early 1980s by the French company Roussel Uclaf • while investigating glucocorticoid receptor antagonists, they discovered compounds that blocked the similarly shaped progesterone receptor. Further refinement led to the production of RU 486 • Clinical testing of mifepristone as a means of inducing medical abortion began in France in 1982. Results from these trials showed that when used as a single agent, mifepristone induced a complete abortion in up to 80% of women up to 49 days’ gestation. • Addition of small doses of a prostaglandin analogue (=> see misoprostol) a few days later to stimulate uterine contractions, a complete medical abortion is achieved in nearly 100 percent of women • approved in the US in 2000 for the termination of early pregnancy (defined as 49 days or less)
Sex Steroids • Male reproductive system • Gonadotropin Releasing Hormone(GnRH) = Gonadoliberin stimulates release of • Follicle stimulating hormone (FSH)(Stimulates Sertoli cells => promotes gametogenesis) and • Luteinising Hormone (LH) = Interstitial Cell Stimulating Hormone (ICSH) which triggers production of • Testosterone (T) (by Leydig cells) which in turn negatively regulates • Pituitary and Hypothalamus hormone production
Sex Steroids Androgens • Testosterone • Primary androgen in humans • Possesses androgenic and anabolic effects: Androgenic effects: • Growth and development of male sex organs • Important for (male) sex drive and performance • Development of secondary sexual characteristics • Important role in spermatogenesis Anabolic effects: • Development of muscle mass • Reverse catabolic or tissue-depleting processes • Dihydro-Testosterone • Active metabolite • Mediates most of testosterone actions
R Sex Steroids Androgens • Testosterone • Hepatic elimination after oral administration • Also short half-life after injection => ester derivatives: Proprionate, enanthate, cypionate… • Fluoxymesterone • Hepatic elimination after oral administration
Sex Steroids Anabolic Androgens Testosterone derivatives: anabolic effects dominant • Nandrolone • Injection • Stanozolol • oral administration
Sex Steroids Anabolic Androgens • Dehydroepiandrosterone (DHEA) • Popular item in health food stores: DHEA was prescription only until recently when changes in federal law labeled it as a nutritional supplement (DHEA sales now equal that of melatonin) • Is actually a testosterone precursor • Supposedly by maintaining youthful DHEA levels one can improve mood, memory, energy and libido, while preserving lean body mass and counteracting the effects of stress hormones. • DHEA may have serious side effects: • If it abnormally increases testosterone, then testosterone side effects may be expected, including acne, testicular atrophy and increased risk of prostate cancer. • Women taking excessive doses of DHEA have reported acne and facial hair. • DHEA can also be converted into estrogen, so high levels of DHEA can lead to estrogen side effects as well, including gynaecomasty and increased risk of breast cancer. • DHEA is often marketed as an anabolic steroid: This is misleading since as an androgen precursor its metabolism will produce testosterone which has anabolic properties
Sex Steroids Anti-Androgens • Flutamide • Non-steroidal receptor antagonist • Used in prostate cancer treatment • Finasteride • Inhibits 5a-reductase => prevent conversion of testosterone into the more potent dihydrotestosterone (DHT) • Used to treat prostate gland enlargement and hair loss (bald man have higher average levels of DHT)
Sex Steroids GnRH analogs/modifiers • Danazol • Inhibits GnRH release => no FSH/LH production => no steroid production • Used to treat endometriosis (growth of endometrial tissue outside of the uterus) • Synthetic GnRH (Gonadorelin, Buserelin, Leuprorelin…) • Up to 200x more potent than GnRH • If given in pulses (s.c.) stimulate gonadotropin release => induce ovulation • If given continously they desensitize the GnRH receptors => gonadal suppression (“medical castration”) • Used in sex hormone-dependent conditions (prostate, breast cancer; endometriosis; uterine fibroids…) • Side effects: menopausal symptoms
Sex Steroids Oral Contraceptives • History • 1937: Investigators demonstrated that the female hormone progesterone could halt ovulation in rabbits • 1949: Scientists at the University of Pennsylvania achieved the production of synthetic progestins • 1953: Margaret Sanger, Katherine McCormick and Gregory Pincus team up to develop a reliable contraceptive • 1950s: Large scale testing of “the pill” was successful • 1960: FDA approves first oral contraceptive (Early pill formulations contained up to 150 micrograms (mcg) of estrogen!) • 1982/84: Introduction of the bi- and tri-stage formulation • 1988: FDA recognized several severe long-term side effects (high estrogen!) • Currently used by 16 mill. women in the US (40% of women between 18 and 24
Sex Steroids Oral Contraceptives Either combination estrogen/progesterone of progesterone alone • Combination pills: • Highly effective • Estrogen component is mostly ethinylestradiol, sometimes mestranol • Progesterone component varies • 21 day cycle with 7 day break (causes withdrawal bleeding) • Can be mono- or biphasic Mechanism: • Estrogen inhibits FSH secretion (neg. feedback loop!) => suppression of follicle development • Progesterone inhibits LH secretion (neg. feedback loop!) => inhibition of ovulation; also increases mucus viscosity • Both steroids alter endometrium => prevent implantation
Sex Steroids Oral Contraceptives Estrogen Progesterone
Sex Steroids Contraceptives • “Mini Pill”: • Contains only a progesterone (Levonorgestrel, Ethynodiol…) • Used when estrogen in contraindicated (e.g. thrombosis) • Taken daily without interruption • Acts mainly by increasing viscosity of mucus (Mucolytica in cough medicine can cause failure) • Less reliable than combination pill • Postcoital contraceptives (“Morning after pill”) • High dose of progesterone (Levonorgestrel) • Must be taken within 72 hrs • Nausea and vomiting are common side effects • Depot and patch formulations • Injection of oily depot formulations every 3 month • Transdermal delivery systems
Sex Steroids Oral Contraceptives Side effects: • Thrombosis • Hypertension • Intermittent bleeding • Weight gain • Depression • Nausea • Loss of libido Drug interactions: • Steroids are metabolized by P450 enzymes • Minimal dose of steroid is used to prevent risk of thrombosis • Any increase in clearance by P450-inducing drugs can result in contraception failure • Frequent cause of OC failure is diarrhea (diminished time for absorption)