Download
1 / 41
460 likes | 921 Vues
Epidemic Encephalitis B. Dept. Of Infectious Disease Shengjing Hospital CMU. Definition. Epidemic encephalitis B is acute infectious disease caused by encephalitis B virus,usually occurs in summer &fall.The virus is transmitted by mosquito. Pathologic lesions: cerebral parenchyma

E N D
Epidemic Encephalitis B Dept. Of Infectious Disease Shengjing Hospital CMU
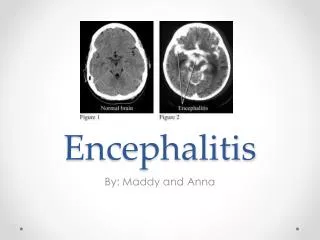
Definition • Epidemic encephalitis B is acute infectious disease caused by encephalitis B virus,usually occurs in summer &fall.The virus is transmitted by mosquito. • Pathologic lesions:cerebral parenchyma • Clinical feature:highfever • altered consciousness • convulsion • meningeal irritation • respiratory failure
Etiology • Causative agent: encephalitis B virus genus flavivirus of flaviviridae • single strain of positive-sense RNA, • virion is spheric, diameter: 15 ~ 22nm, • Resistance: unstable in environment, • Sensitive to heat, disinfectants, • ultraviolet rays
Etiology • antigenicity: stable • hemagglutination inhibiting Ab • complement fixing Ab • neutralizing Ab
Epidemiology • Source of infection domestic animals: pig, horse, dog poultry: chicken, duck, goose. patients:
Epidemiology • Route of transmission insect borne: mosquito biting , vector: mosquito, culex tritaeniorhynchus. Survived winter mosquitoes pigs mosquitoes mosquitoes person pigs
Epidemiology • Susceptibility of population: • universal susceptible • lifelong immunity • subclinical infection : overt infection 1000~2000:1
Epidemiology • Epidemiologic features • sporadic from July to Sep. • children under 10yrs (2~6yrs) • hypersporadic property
virus mosquito biting replication in mononuclear-phagocyte system (MPS) blood stream brief viremia blood-brain barrier clearance CNS subclinical inf. onset of illness No. of virus of invasion cellular immunity blood brain barrier
Pathology • Place of lesion: • all of CNS • cerebral cortex, midbrain and thalamus . • Pathologic features • gross examination: • congestion • hemorrhage • cerebral edema • soften focuses
Pathology • microscopic examination: • vascular lesion: endothelial cells swelling, necrosis • neuron degeneration & necrosis • neurogliocyte hyperplasia & inflammatory cells infiltration, perivascular cuffing , neuronophagia.
Clinical manifestation • incubation period:10~14 days (4~21days ) • typical encephalitis B • Initial period • crisis period • convalescent period • sequela period
Clinical manifestation • Initial period : on the 1st to 3rd days • abrupt onset • fever with headache , nausea, vomiting lethargy, • abdominal pain , diarrhea,
Clinical manifestation • Crisis period- on the 4th ~10th days • high fever: >40℃, sustained for 7~10 days. • altered consciousness: lethargy, confusion, delirium, stupor, semicoma, coma. • convulsion or twitch:(40~60%) • respiratory failure: 15~40%
Clinical manifestation • central RF: • reason of central RF: • lesion of cerebral parenchyma (respiratory center injury in oblongata medulla) • cerebral edema • brain hernia • intracranial hypertension • hyponatremic encephalopathy
Clinical manifestation • manifestation of central RF: • cacorhythmic breathing (cheyne-stokes breathing, apnea) • brain hernia • peripheral RF: • dyspnea, regular breathing
Clinical manifestation • Other symptoms & signs of CNS • meningeal irritations (neck stiffness Kernigs & Brudzinskis signs positive) • Deep tendon reflexes from hyperactive to disappear • pathologic reflexes positive • limbs paralysis
Clinical manifestation • Convalescent period • T drop to normal in 2~5 days • neurologic function regain gradually(2W) • remain some behavioral & psychologic abnormalities, aphasia, dementia, rigidity paralysis. • >6month - sequela
Clinical manifestation • Sequela period • aphasia • dementia • persistent paralysis
Clinical manifestation • Clinical type: • mild type • common type • severe type • fulminant type
Laboratory Findings • Blood picture: WBC 10~20×109 /L neutrophil >80% • Cerebrospinal fluid- aseptic meningitis • transparent or slightly cloudy, • pressure may be elevated • pleocytosis: 50~500×106/L • protein may be elevated mildly • glucose and chloride are normal
Laboratory Findings • Serological test: • specific IgM Ab: blood or CSF, 3~4d after onset, peak on 2 week ELISA or indirect immunofluorescence • complement fixing Ab: 2 weekafter onset, peak on 5~6 week, • anamnestic diagnosis • epidemiologic investigation
Laboratory Findings • hemagglutination inhibition Ab: 5d after onset, peak on 2 week • diagnosis: 4 fold increase in titer • epidemiologic investigation • neutralized Ab epidemiologic investigation
Laboratory Findings • pathogenic test virus isolation:blood, CSF, brain tissue RT-PCR : RNA
Diagnosis • Epidemiological data: • 7~9 month • <10yrs • Clinical manifestation: fever, headache, vomiting, altered consciousness, convulsion, meningeal irritation, pathologic reflexes positive. • Laboratory findings:WBC, CSF, IgM
Differential Diagnosis • toxic bacillary dysentery high fever,convulsion,coma. • <24h • circulatory failure: early • stool examination: WBC, RBC • CSF: normal • meningeal irritation: negative
Differential Diagnosis • tuberculous meningitis • CSF, meningeal irritation • purulent meningitis • other viral encephalitis
Treatment • General therapy: • Isolation: preventing mosquito biting, T<30℃ • nursing: mouth, skin, eye, turn over clapping back sputum aspiration
Treatment • fluid & electrolyte supplementation adult: 1500~2000ml/d children: 50~80ml/kg/d • Symptomatic therapy • high fever: T<38℃
Treatment • physical cooling (ice bag, alcohol bathing, cold saline enema) • drug cooling antipyretic subhibernation: chlorpromazine 0.5~1mg/kg/time phenergan 0.5~1mg/kg/time 4~6h, 3~5day
Treatment • convulsion: fever: cooling brain edema: 20% mannitol 1~2g/kg/time 50% glucose dexamethason
Treatment sedative: valium: adult:10~20mg/time children: 0.1~0.3mg/ kg/ time 10% chloral hydrate: adult:1~2g/time children: 60~80mg/kg/time subhibernation:
Treatment • respiratory failure: • keep airway clear • sputum aspiration • turn over , clapping back, postural drainage • aerosolization • inhalation of oxygen
Treatment • reducing cerebral edema & hernia dehydrate : 20% mannitol :1~2g/kg/time 50% glucose , • vasodilator: 654-2: adult: 20mg/time children: 0.5~1mg/kg/time 10~30 min
Treatment • respiratory stimulant: lobeline: adult: 3~9mg/time children: 0.15~0.2mg/kg/time coramine: adult: 0.375~0.75g/time children: 5~10mg/kg/time • tracheal intubation or tracheotomy, biomotor
Treatment • Convalescent & sequela period • acupuncture • massage • exercise etc.
Prevention • isolating patients and pig immunization, • killing mosquito and preventing mosquito , • vaccination: killed virus vaccine: 60~90%
病例分析 5岁患儿,8月15日开始发热头痛,呕吐一次,次日排稀便两次,精神不振,第三天晚间开始抽搐,神志不清。查体,T40℃,急病容,脉充实有力,呼吸略促,节律整,皮肤无瘀点、瘀斑,颈强(+),克氏征(+),肢体肌张力增强。辅助检查:
病例分析 • 血WBC 15×109/L,便常规WBC 0~5个/Hp, CSF细胞数75×106/L,糖3.5mmol/L,氯化物115mmol/L,蛋白0.45g/L • 哪种诊断可能性大? • 提供诊断依据及主要鉴别诊断 • 治疗要点