Download
1 / 1
10 likes | 162 Vues
Use of Emergency Facilities for the Treatment of Neisseria gonorrhoeae Infection in the United States. Newman L 1 , Donnelly J 2 , Marcus J 3 , Martins S 4 , Stenger M 5 , Stover J 6 , Nelson R 1 , Weinstock H 1 , on behalf of the STD Surveillance Network SSuN

E N D
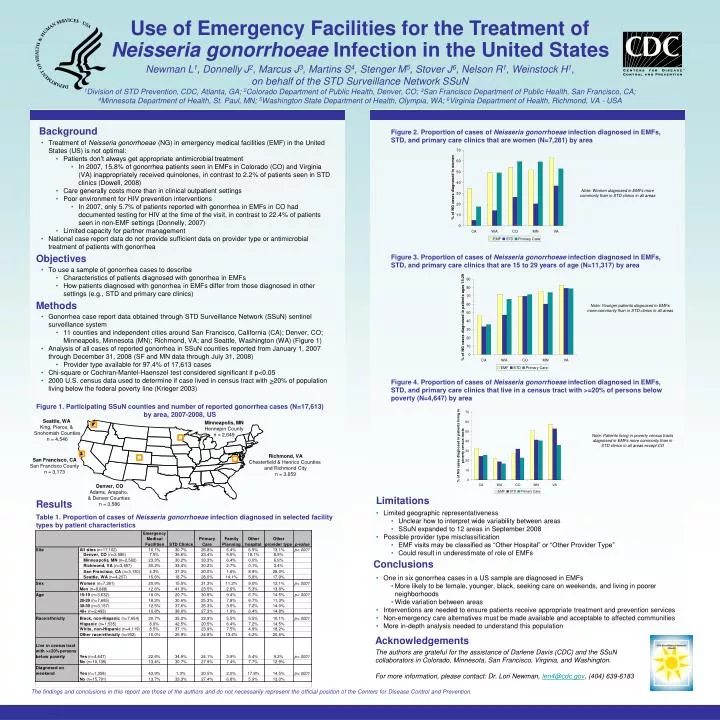
Use of Emergency Facilities for the Treatment of Neisseria gonorrhoeae Infection in the United States Newman L1, Donnelly J2, Marcus J3, Martins S4, Stenger M5, Stover J6, Nelson R1, Weinstock H1, on behalf of the STD Surveillance Network SSuN 1Division of STD Prevention, CDC, Atlanta, GA; 2Colorado Department of Public Health, Denver, CO; 3San Francisco Department of Public Health, San Francisco, CA; 4Minnesota Department of Health, St. Paul, MN; 5Washington State Department of Health, Olympia, WA; 6Virginia Department of Health, Richmond, VA - USA Background Figure 2. Proportion of cases of Neisseria gonorrhoeae infection diagnosed in EMFs, STD, and primary care clinics that are women (N=7,281) by area • Treatment of Neisseria gonorrhoeae (NG) in emergency medical facilities (EMF) in the United States (US) is not optimal: • Patients don’t always get appropriate antimicrobial treatment • In 2007, 15.8% of gonorrhea patients seen in EMFs in Colorado (CO) and Virginia (VA) inappropriately received quinolones, in contrast to 2.2% of patients seen in STD clinics (Dowell, 2008) • Care generally costs more than in clinical outpatient settings • Poor environment for HIV prevention interventions • In 2007, only 5.7% of patients reported with gonorrhea in EMFs in CO had documented testing for HIV at the time of the visit, in contrast to 22.4% of patients seen in non-EMF settings (Donnelly, 2007) • Limited capacity for partner management • National case report data do not provide sufficient data on provider type or antimicrobial treatment of patients with gonorrhea Note: Women diagnosed in EMFs more commonly than in STD clinics in all areas Objectives Figure 3. Proportion of cases of Neisseria gonorrhoeae infection diagnosed in EMFs, STD, and primary care clinics that are 15 to 29 years of age (N=11,317) by area • To use a sample of gonorrhea cases to describe • Characteristics of patients diagnosed with gonorrhea in EMFs • How patients diagnosed with gonorrhea in EMFs differ from those diagnosed in other settings (e.g., STD and primary care clinics) Methods Note: Younger patients diagnosed in EMFs more commonly than in STD clinics in all areas • Gonorrhea case report data obtained through STD Surveillance Network (SSuN) sentinel surveillance system • 11 counties and independent cities around San Francisco, California (CA); Denver, CO; Minneapolis, Minnesota (MN); Richmond, VA; and Seattle, Washington (WA) (Figure 1) • Analysis of all cases of reported gonorrhea in SSuN counties reported from January 1, 2007 through December 31, 2008 (SF and MN data through July 31, 2008) • Provider type available for 97.4% of 17,613 cases • Chi-square or Cochran-Mantel-Haenszel test considered significant if p<0.05 • 2000 U.S. census data used to determine if case lived in census tract with >20% of population living below the federal poverty line (Krieger 2003) Figure 4. Proportion of cases of Neisseria gonorrhoeae infection diagnosed in EMFs, STD, and primary care clinics that live in a census tract with >=20% of persons below poverty (N=4,647) by area Figure 1. Participating SSuN counties and number of reported gonorrhea cases (N=17,613) by area, 2007-2008, US Seattle, WA King, Pierce, & Snohomish Counties n = 4,546 Minneapolis, MN Hennepin County n = 2,649 Note: Patients living in poverty census tracts diagnosed in EMFs more commonly than in STD clinics in all areas except CO Richmond, VA Chesterfield & Henrico Counties and Richmond City n = 3,659 San Francisco, CA San Francisco County n = 3,173 Denver, CO Adams, Arapaho, & Denver Counties n = 3,586 Limitations Results • Limited geographic representativeness • Unclear how to interpret wide variability between areas • SSuN expanded to 12 areas in September 2008 • Possible provider type misclassification • EMF visits may be classified as “Other Hospital” or “Other Provider Type” • Could result in underestimate of role of EMFs Table 1. Proportion of cases of Neisseria gonorrhoeae infection diagnosed in selected facility types by patient characteristics Conclusions • One in six gonorrhea cases in a US sample are diagnosed in EMFs • More likely to be female, younger, black, seeking care on weekends, and living in poorer neighborhoods • Wide variation between areas • Interventions are needed to ensure patients receive appropriate treatment and prevention services • Non-emergency care alternatives must be made available and acceptable to affected communities • More in-depth analysis needed to understand this population Acknowledgements The authors are grateful for the assistance of Darlene Davis (CDC) and the SSuN collaborators in Colorado, Minnesota, San Francisco, Virginia, and Washington. For more information, please contact: Dr. Lori Newman, len4@cdc.gov, (404) 639-6183