Download
1 / 13
150 likes | 392 Vues
CORONARY CIRCULATION-ANATOMY HISTORY. 1650= Vieussens described first. 1799=Edward Jenner established the relationship between the coronary artery and angina pectoris. 1809=Allan Burns described the same. 1958=Maron Sones performed the first selective coronary arteriography.

E N D
CORONARY CIRCULATION-ANATOMYHISTORY 1650= Vieussens described first. 1799=Edward Jenner established the relationship between the coronary artery and angina pectoris. 1809=Allan Burns described the same. 1958=Maron Sones performed the first selective coronary arteriography. 1968=Rene Favalan and Dudley Johnson introduced the coronary artery bypass surgery.
CORONARY ARTERY ANATOMY- DEVELOPMENT • Coronary vascular endothelial maturation-closely parallels the development of embryonic epicardium. • Heart begins to pump blood before perfusion of the coronary vasculature occurs-early trabecular myocardium is metabolically supplied by local diffusion of nutrients.This fact-made use of in endocardial laser revascularisation procedures for angiographically proved extensive disease of the coronary arteries, where CABG is not feasible. • Neural crest ablation-marked abnormality of coronary vessel development.
ANATOMY-CONTD. • Coronary arteries-2 in no. arise from evaginations,coronary sinuses at the root of aorta. Left-from left coronary sinus & Right-from right coronary sinus.The third evagination-non-coronary sinus. Two major and two minor loops. Major loops-situated along the interventricular and AV grooves. Minor loops-around the right ventricular conus and the sinoatrial region. Architectural pattern • Epicardial or conductance vessels. • Intramyocardial or resistance vessels. • Subendocardial plexus of vessels.
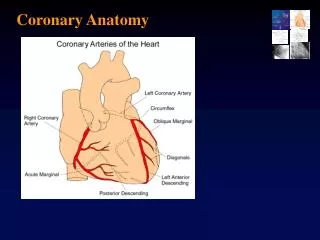
COURSE & BRANCHES • Left coronary-coronary sinus-LAD & circumflex arteries. • LAD= in the interventricular groove till the apex-supplies about 50% of the LV mass and a small strip of the adjoining right ventricle. Branches: a) Septal perforators- supply inter-ventricular septum. b) Diagonals-supply the remaining LV mass. • Circumflex= travels in the left AV groove,finally reaches the crux on the posterior aspect of the heart. Branches: a) obtuse marginals=1-4 in no. and supply the lateral wall of the left ventricle. Left main=sometimes trifurcates. Intermediate artery-supply similar to 1st diagonal. RCA= rt.coronary sinus-right atrioventricular sulcus.-crux-meets terminal portion of circumflex.
Contd. • Right dominant= posterior descending artery from RCA, travels in the posterior interventricular groove. Left dominant=PDA from the circumflex. Branches of RCA: a) conus a.-meets a branch from LAD around the conus of the right ventricle-one minor loop of the coronary circulation. b) sinus node a.->50%=from RCA-opposite direction of conus a.-encircles the SVC-rt. Atrial junction-second minor loop. c) acute marginal branch=travels along the lower border of rt. atrium. d) posterior descending artery=terminal portion communicates with the terminal portion of the LAD artery around the apex.Where there isa major blockade of the LAD, a patent right dominant system can supply the LAD region in a retrograde way.
REGIONAL MYOCARDIAL BLOOD SUPPLY • LV= 50% from the LAD. 25% from the left circumflex, 25%-posterior descending a.(from rt. Coronary or the left circumflex). . The anterolateral papillary muscle-blood supply from the diagonal branches of LAD. The posterior papillary muscle-dual blood flow from circumflex and terminal branches of RCA. Sinus node-In majority by RCA, in a small proportion by the circumflex. AV node-The first posterior perforator of the PDA. Bundle of His-dual blood supply from both the PDA and LAD, more resistant to ischemia than the AV node. Rt. Bundle-LAD and RCA. Left bundle-mainly from the diagonals. RV=Anterior portion adjacent to the interventricular septum-branches of LAD.Rest-RCA. In left dominant-posterior portion -circumflex. RA-RCA. LA-Left circumflex.
VENOUS DRAINAGE An extensive intercommunicating network by a. the coronary sinus b. the anterior right ventricular veins. c. the thebesian veins. Coronary sinus= in the left posterior AV groove-drains predominantly the left ventricle and the left atrium. Tributaries:a)The anterior inter-ventricular vein-ends as great cardiac v b) The middle cardiac vein-from the posterior interventricular region. c) the oblique vein of Marshell-from the posterior aspect of left atrium. - opens into the rt.atrium between the orifice of IVC and septal tricuspid leaflet.
The anterior cardiac v.-2-4 in no. They drain the anterior right ventricular wall and end at the base of the right atrium. • The small cardiac v.-receives from rt.atrium and opens into RA. • The thebesian veins-tiny venous outlets draining the myocardium directly into the cardiac chambers(rt. Atrium and rt.ventricle). INNERVATION Sympathetic: from superior,middle and inferior cervical ganglia+upper 5 ganglia of the symp.chain. Para-symathetic: nodose ganglion. At the heart, both mingle to form cardiac plexus-superficial and deep portion. Compared to the symathetic, the parasympathetic innervation is sparse.
Distribution of blood volume and O2 consumption • 5% of the blood flow of the total cardiac output(250-275ml/min). • AV oxygen content difference=10 ml/100 ml(5 ml/100 ml in other vascular beds). • During exercise, the values are the same. • Oxygen consumption-25 ml/min.(beating heart at rest). -6 ml/min(non-beating heart). -0.12 ml/min(for electrical activation)]
REGULATION OF THE CORONARY BLOOD FLOW • Anatomical factor: arranged as a) epicardial conductance vessels (constrict to alpha stimulation and dilate to NTG.) b) intramyocardial resistance vessels(at right angles to the above). c)subendocardial plexus of vessels-dense capillary network of about 4000 capillaries/sq.mm, not uniformly patent-pre-capillary sphincters serve a regulatory role-opens out when myocardial demand increases. • Perfusion pressure: LV perfusion pressure= aortic diastolic pressure- LV end-diastolic pressure. All organs are perfused during systole except the LV(since the resistance vessels are compressed during systole). RV-thinner ventricle. Receives its major blood flow during systole.
REGULATION OF BLOOD FLOW-CONTD. • Under basal conditions, blood flow to the subendocardium/subepicardial layer=125:1 (maximal preferential dilatation of the subendocardial plexus of vessels. • Significance: In the presence of a significant coronary artery obstruction, subendocardial vessels can’t dilate further and suffer the most by way of ischemia. • Collaterals: Anastomotic connections between portions of the same coronary artery and between different coronary arteries-diameter-40-200 µ. Open out only with repeated brief periods of ischemia.With sustained partial occlusion-collateral blood flow commences in 5-10 min. and progressively increases for 24 hrs.In 6-12 months time , they acquire an organised smooth muscle coat.They are influenced by external influences. • Significance: No anginal pain even with 80-90% obstruction of a major vessel but when demand is increased, collateral circulation may be inadequate.
CONTROL OF CORONARY VASCULAR RESISTANCE • Local metabolism: primary controller. Local arterial vasodilatation in response to muscle need for nutrition. Chemical agents resposible are: • a) adenosine • b) potassium ions • c) hydrogen ions • d) bradykinin • e) prostaglandins.PGI2 and PGE2. • Oxygen lack: opening of ATP dependent K+ channels-hyper-polarization- Ca2+ channel opening prevented-vasodilatation. • Auto-regulation:At perfusion pressures from 60-130 mm of Hg, CBF is the same(myogenic, metabolic factor and release of endothelial vaso-active factors are implicated). • Neural factor: α-vaso-constriction ß-vaso-dilatation. Para symp-dilates • Endothelial control: EDRF(released by several stimuli), prostacyclin, endothelin.
TERMINOLOGIES • Reactive hyperemia • Coronary flow reserve • Coronary steal • Myocardial stunning • Myocardial hybernation Deteminants of Myocardial oxygen demand & supply Supply ↓: a) Coronary stenosis Demand ↑: a)Heart rate b) Coronary perfusion pressure↓ b)contractility c) ↓coronary perfusion time c)ventricular d)↓Hb wall tension e)↓PaO2. d)ventricular cavity radius