Download
1 / 39
410 likes | 648 Vues
AUTONOMIC NERVOUS SYSTEM. DR. MUNISHA AGARWAL DR. SAURABH TANEJA. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. PARASYMPATHETIC Long preganglionic fibers Short postganglionic fibers Function : Conserves energy 1 preganglionic synapses with 1 postganglionic fibre . SYMPATHETIC

E N D
AUTONOMIC NERVOUS SYSTEM DR. MUNISHA AGARWAL DR. SAURABH TANEJA www.anaesthesia.co.in anaesthesia.co.in@gmail.com
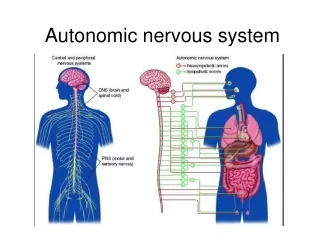
PARASYMPATHETIC Long preganglionic fibers Short postganglionic fibers Function : Conserves energy 1 preganglionic synapses with 1 postganglionic fibre SYMPATHETIC short preganglionic fibers long post ganglionic fibers Function : fight/ flight response one preganglionic synapses with many postganglionic fibres SYMP. & PARASYMP. NS.
PARASYMPATHETIC Neurotransmitter : acetylcholine Both @ preganglionic & postganglionic SYMPATHETIC acetylcholine @ preganglionic & norepinephrine @ postganglionic except sweat glands & some skeletal muscle blood vessels : norepinephrine SYMP. & PARASYMP. NS.
PARASYMPATHETIC Cranial nerves III, VII, IX, X, bulbar portion of XI , S2,3,4 (craniosacral) CN III to eye, CN VII to lacrimal, nasal and submaxillary glands., CN IX to parotid glands; vagus to heart, lungs, oesophagus, stomach, small intestine, liver, gall bladder pancreas & upper part of the uterus the sacral part innervates distal colon, rectum, bladder, lower portions of uterus & external genitalia SYMPATHETIC T1 – L2 (thoracolumbar) 22-24 ganglia on each side cervical (3), thoracic (10-12), lumbar (4), sacral (4,5) ganglion impar T1 to head, T2 to neck & heart, T3- T6 to chest, T7-T11 to abdomen, T12-L2 to legs
NON INVASIVE TESTS FOR ASSESSING THE AUTONOMIC NERVOUS SYSTEM • PARASYMPATHETIC Tests involving changes in the heart rate measure injury to parasympathetic system • SYMPATHETIC After changes in HR, changes occur in the measures of Blood pressure that reflect sympathetic injury.
VALSALVA MANOUVER • checks baroreflex control of HR (parasympathetic) & the BP (adrenergic) • PHASES I & II ARE DURING BREATH HOLDING • PHASES III & IV AFTER RELEASE • The BP & HR responses are mirror images • Phase I : brief rise in BP due to increased intrathoracic pressure constricting the great vessels • Phase II : gradual fall in BP impaired venous return, causing decreased stroke volume & decreased BP that reaches a plateau because of peripheral vasoconstriction i.e. increased systemic vascular resistance, with a compensatory tachycardia
Phase III : brief fall in BP because of removal of intrathoracic pressure constricting the great vessels • Phase IV : occurs after valsalva is released & patient resumes normal breathing, BP begins to rise. After 15-20 sec. there is a rebound overshoot of BP to above baseline (due to persistent peripheral arteriolar vasoconstriction and increased cardiac adrenergic tone), accompanied by reflex bradycardia, with heart rate below baseline for about 1 min.
Valsava ratio can be calculated & age specific references seen. It is a measure of cardiovagal function. • A lack of rebound overshoot of BP during phase IV is an early indicator of autonomic dysfunction. • Practical help : this rebound overshoot in phase IV, however, can be detected by inflating a cuff to just at SBP and then having the patient valsalva. Without changing the cuff pressure, the sounds will disappear during breath holding , and on release the sounds will reappear and can be followed up to detect the rebound overshoot in BP.
ORTHOSTATIC HYPOTENSION • Defined as a sustained drop in SBP (≥ 20 mm Hg) or DBP (≥ 10 mm Hg) within three minutes of standing. • In non neurogenic causes, it is accompanied by a compensatory increase in HR > 15/min. an important clue to a neurogenic cause is aggravation or precipitation of symptoms by autonomic stressors (meal, hot bath, exercise, alcohol consumption). • allow 20 minute period of supine rest before assessing changes in BP during tilting.
BLADDER • detrusor muscle innervated by parasympathetic neurons located at S2-S4 level. • internal urethral sphincter innervated from T12-L1 level via sympathetic prevertebral plexus and the hypogastric nerve. • Normal micturition requires intact autonomic nervous system spinal pathway cerebral inhibition control of external sphincter
LESIONS CEREBRAL CORTEX : • Loss of inhibition. Bladder tone is normal. • Micturition occurs by stretch reflex. • Signs & symptoms are frequency, urgency, hesitancy, incontinence. Bladder sensation is normal. • There is no residual urine.
REFLEX NEUROGENIC BLADDER: • Occurs with severe myelopathy & extensive brain lesions causing interruption of both the descending autonomic tracts to the bladder & ascending sensory pathways above the sacral segments of the cord. • Bladder capacity is small & micturition reflex is reflex & involuntary. Residual urine volume is variable.
AUTONOMOUS NEUROGENIC BLADDER • It is without external innervation. • Sensation is absent. There is destruction of parasympathetic supply. • no reflex or voluntary control of the bladder. Contractions occur as the result of stimulation of the intrinsic neural plexuses within the wall. • Amount of residual urine is large but the bladder capacity is not greatly increased.
SENSORY PARALYTIC BLADDER • Lesions in the posterior root or the posterior root ganglia of the sacral nerves or the posterior columns of the spinal cord. • Sensation is absent and there is no desire to void. • There may be distension, dribbling, and difficulty both in initiating micturition & emptying the bladder. • There is large amount of residual urine.
MOTOR PARALYTIC BLADDER • Motor nerve supply is interrupted. • The bladder distends & decompensates but sensation is normal. • The residual urine & bladder capacity may vary.
SEXUAL FUNCTION • Erection is a parasympathetic function, S2-S4 • Ejaculation is a sympathetic function, lumbar nerves. • Autonomic insufficiency usually causes impotence but pathological exaggeration of sexual reflex may occur as a part of mass reflex which may produce priapism. • In autonomic neuropathy, especially from diabetes, retrograde ejaculation (lack of closure of internal vesical sphincter during ejaculation; producing milky white urine ) may procede the development of impotence.
RECTUM • If sacral segments or pelvic nerves involved; laxity of the sphincters & incontinence may occur • Gripping of the gloved finger by the internal sphincter will be absent. • Stroking the skin near the external sphincter will not produce reflex contraction • Higher spinal or pontine lesions : tonic contraction of the sphincters & result in constipation
IMPAIRED GLANDULAR ACTIVITY • Difficulty in food intake due to decreased salivation • Eye irritation due to decreased lacrimation • Decreased sweating causing temperature elevation and vasodilation
SUDOMTOR & THERMOREGULATORY FUNCTION • Abnormal dryness of skin may be sign • Lack of normal moisture in the socks may indicate • Localized : peripheral nerve injury • Generalized : diffuse dysautonomia • Simple bedside test : stroking of the skin with the finger/ pen or spoon Smoothly : dry (sympathectomised) Irregularly/ unevenly : moist, perspiring skin
Various tests are sympathetic skin response (SSR), Quantitaive sudomotor axon reflex test (QSART), sweat imprint, thermoregulatory sweat test (TST) • SSR assesses peripheral sympathetic function by detecting changes in skin resistance in response to sudomotor discharges. • TST assesses both the central & peripheral sympathetic components by analyzing the sweating response to rise in body temperatures
QSART assesses the postganglionic sudomotor fibers by measuring the sweat output in response to iontophoresis of acetylcholine into the skin. • sweat imprint test quantifies the sweat output by visualizing the imprints sweat droplets make on a plastic or silicon mould. • TST combined with a test of postganglionic function can localize the site of process causing anhidrosis. • If the postganglionic function test is abnormal, the cause is postganglionic. But if the postganglionic test is normal and the TST is abnormal, the cause is preganglionic
TEAR PRODUCTION • SCHIRMER TEST : placing a strip of sterile filter paper in the lower conjunctival sac and measuring the degree of wetting over 5 minutes.
PHARMACOLOGICAL TESTS • Measurement of plasma NE first with patient supine and then after standing for atleast 5 min. supine values are decreased in postganglionic disorders (autonomic neuropathy or pure autonomic failure) and may fail to increase in preganglionic or postganglionic disorders (e.g. multiple system atrophy).
To evaluate postganglionic adrenergic function, tyramine (releases NE from postganglionic terminals) and phenylephrine (denervation supersensitivity- directly acting α1 agonist) used. In a postganlionic lesion, the response to tyramine is reduced & there is excessive response to subthreshold doses of phenylephrine. • Other strategies include ganglionic blockade with trimethaphan (greater fall in resulting BP with a preganglionic lesion) or administration of arginine vasopressin (to evaluate afferent central pathways).
DIABETES MELLITUS • Most common cause of autonomic neuropathy • Earliest autonomic instability is loss of vagal controlled heart rate variability with deep breathing, decreased peripheral sympathetic tone with increase in blood flow & loss of distal sudomotor function, detected by QSART. • In advanced disease, signs of autonomic dysfunction involving cholinergic, noradrenergic & peptidergic systems
CVS : resting tachycardia, orthostatic hypotension (loss of baroreceptor reflex), sudden death, ↓ BP @ induction ↑ need for vasopressors • GIT : gastroparesis, nocturnal diarrhea common (parasympathetic dysfn RSI required) • GU : Cystopathy (inability to sense full bladder and failure to void completely leading to urinary hesitancy, decreased voidingfrequency, incontinence & UTI); erectile dysfunction (increases with age and duration of disease); retrograde ejaculation
SUDOMOTOR : hyperhidrosis in the upper limb & anhidrosis in the lower limbs leading to cracking & increased chances of foot ulcers. in diabetic foot; pain & temp senses are lost before loss of touch & vibration senses. • METABOLIC : typical signs & symptoms of hypoglycemia may not appear because damage to sympathetic innervation of the adrenal gland can result in lack of epinephrine release (hypoglycemia unawareness)
AGING • Orthostatic hypotension common (dec. baroreceptor reflexes) • Decreased vagal function & increased NE conc. are balanced by compensatory downregulation of β1 adrenoreceptors • Loss of control leading to increase in CHF incidence
SPINAL CORD TRANSECTION • In paraplegic patients, small stimuli may evoke exaggerated sympathetic discharges • remember the vagus is intact in quadriplegics; may stimulate it by tracheal suctioning & response ↑ by hypoxemia • as Symp NS inactive; overactivity of RAA system; so use ACEI cautiously.
bladder or bowel distension mass reflex ↑ BP, ↓ flow to periphery, flushing & sweating above the lesion & ↓ HR • over sensitive to angiotensin & catecholamines • monitor temperature during anesthesia as hypothermia due to inabiity to shiver & cutaneous vasodilation or hyperthermia due to loss of normal sweating response, may occur
THANKS www.anaesthesia.co.in anaesthesia.co.in@gmail.com