Download

1 / 37
370 likes | 455 Vues
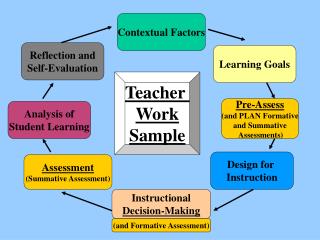
Insight, creates meaning, judgmental, actionable Human, tacit, transfer requires learning. Wisdom. Knowledge. Information. Contextual Codifiable, explicit Easily transferable. Data.

E N D
Insight, creates meaning, judgmental, actionable Human, tacit, transfer requires learning Wisdom Knowledge Information Contextual Codifiable, explicit Easily transferable Data
The location & design of treatments areas are changing within the hospital facilities, as free-standing and mobile treatment sites are evolving. Healthcare benefits, coverage, choices, and costs are continuing to evolve. Hospitals are being subjected to more pressure to manage costs. Hospitals and healthcare centers are treating older adults and younger prematurely born infants, both group having higher acuity level.
Hospitals are developing technology Planning and construction project management programs to guide their decisions because limited resources are being subjected to competing demands, thus requiring more carefully executed plans Technology planning and Acquisitionsteams are created to coordinate the absorption of new and replacement technologies that can contribute to a cost-effective delivery of quality care, these teams may also suggest changes in the current delivery system.
Over the coming years, Saudi Arabia is expecting a significant increase in the demand for healthcare driven by • Rapidly growing and maturing population • Drive to improve the quality of healthcare services in the Kingdom • Today, the Saudi healthcare system is mainly funded by the Government –around 75% of the Kingdom’s overall healthcare expenditures are Government funded • The Ministry of Health (MoH) has prepared a plan to fundamentally restructure its activities, and by so doing, the healthcare sector as a whole • The Ministry will become a healthcare regulator, plus provider of primary care • The Ministry’s hospital assets will be transferred to an independent entity, initially owned by the Government, thus paving the way for more extensive Public Private Partnerships (PPPs) in healthcare • A national fund will be established under the Ministry of Finance to pay for healthcare services provided to patients • This increasing demand for healthcare, changes in the structure of the healthcare industry, and more extensive private sector participation, are expected to lead to a significant increase in investment opportunities in healthcare
Population Growth and Corresponding Healthcare Demand Projections Saudi Population Growth Projections (in Millions) (2005 – 2016) Bed Demand Projections (in 1000s) (2005 - 2016) High-level projections based on extrapolation of current indicators Estimated CAGR (2005-2016) 20% Projections of Demand for Physicians (in 1000s) (2005 - 2016) Estimated Budget allocation ( 1 billion)(2005-2016) 2.4% Projections of Number of Hospital (2005 - 2016) Source: Saudi Ministry of Economy & Planning, Central Department of Statistics, MoH Statistics
Examples of Health System Future Pressure Points Partial List Average Body Mass Index (BMI) of Saudi nationals, 15 years and above, is about 30 kg/m2 – global average BMI is 23; a BMI score greater than 25 are considered overweight Expenditures on cardiovascular diseases are expected to quadruple in the next 20 years The spread of tobacco use in Saudi Arabia among adult males represents 24%; smoking among school children and adolescents exceeds 14% among males Expenditures on cancer treatment is expected to triple in the coming 20 years Mainly arising from a very high rate of consanguinity – roughly 31% of couples in Saudi Arabia are related by blood About 25% of the overall Saudi population over 20 years old are diabetic, compared with 5% globally. The Kingdom currently spends in excess of SR 4 billion on diabetes care – spending expected to triple in the coming 20 years The percentage of elderly people above the age of 60 years old is expected to more than double from the current ~1 million people (4% of the population) to roughly~2.5 million (or 7% of the population) by 2020 Economic development, enhanced patient awareness, more demanding patients, plus the availability of more advanced (and expensive) care will generate upward pressures on healthcare expenditures Obesity & Cardio-vascular Diseases Lifestyle Factors Smoking / Cancer Type I and II Diabetes Other Chronic Diseases Blood-borne Illnesses Aging Population Other Factors Evolving Patient Expectations Source: MoH press releases, literature search
Grade A A A A B B B B C C C C D D E E Healthcare System Quality Rating (2005) Basis of Ratings • A-High quality care, good average health status • Overwhelming majority of the population has access to a high standard care • Health system is well balanced between primary, secondary and tertiary care • B- Good quality care, good average health status • Overwhelming majority of the population has access to good care, although services are stretched • Healthcare expenditure is high, but insufficient to be close to meeting demand • C- Mixed quality of care, mixed average health status • Most of the population has access to some form of care, although the quality of that care is mixed • Services often very stretched and a lack of doctors and facilities, particularly in rural areas • D-Struggling health service, poor average health status • Lack of doctors and health facilities • Significant variations in access to healthcare • E-Dysfunctional health system, extremely poor average health status • Short supply of doctors and health facilities, especially outside urban conglomerations • Significant variations in access to care, with a large proportion of the population lacking easy access
Ministry of Health Capacity Development Program • SR44.4 billion (~$12 billion) spending on healthcare and social services, up 13% relative to 2007 • 79 hospitals under construction • 8 new hospitals • 250 primary care centers to be developed
Patient Healthcare Delivery Service Funding Regulation Degree of Government Ownership Degree of Private Sector Ownership Saudi Arabia Best-in-Class / Desired Health System Position Level 2: “Emerging” Health System Level 1: “Gov’t-Sponsored” Health System Level 3: “Intermediate” Health System Level 4: “Market-Driven” Health System Patient Patient Patient Healthcare Delivery Healthcare Delivery Healthcare Delivery Service Funding Service Funding Service Funding Regulation Regulation Regulation • Widespread private sector healthcare delivery options • Public sector provisioning limited to selected patients (e.g. the poor / military) • Increasing healthcare regulations • Predominance of public sector activities– ‘Command and Control’ model • Private sector involvement limited to few care providers • Emerging private sector involvement in healthcare and increasing private insurance • Decreasing burden on gov’t due to private insurance • Mounting pressures for establishing a comprehensive regulatory framework • Near-absence of public sector healthcare • Government role limited to ensuring oversight, with limited subsidies • Comprehensive regulations to ensure fair play Increasing Private Sector Participation
10% 90% 30% 40% 60% 70% Public Sector Participation Private Sector Participation Share of Healthcare Delivery – Number of Beds Comparison (Selected Saudi Cities)(2005) Observations Illustrative 24% • In Jeddah, private sector participation is considerably more advanced than elsewhere in the Kingdom • The health provider system in Jeddah is perceived as being better than other parts of the Kingdom – some patients travel to Jeddah seeking quality care • On the other hand, several regions such as in the South remain lacking in terms of private sector presence 76% Eastern Region Riyadh Region Jeddah Region Southern Region Source: KSA Ministry of Economy & Planning, Central Department of Statistics, MoH Statistics
MoH Modernization Plan MOH Sector Modernization Plan • Issue regulations to implement the plan • Develop preventive and curative primary care activities to be provided by the MOH • Establish General Organization for Hospitals, and transfer the hospital assets of MOH to this organization –the hospitals will continue to be Government owned • Establish National Health Fund separate from MOH (under MOF), to fund directly healthcare services provided to patients • Establish Regional Health Directorates (13), and allocate independent health budget from the Government to each of them • Establish Regional Health Councils to ensure coordination of health activities on a regional basis Source: Balsam – Development of Saudi Healthcare System - 2006
Trailing leads are trip hazards Locked fire exit to Female Surgery Typical internal corrosion within boiler plant Air cooled chillers in poor condition Existing poor clinical flooring Existing defective clinical flooring Existing temporary door signage Existing suspended ceilings Existing defective furniture Defective light fittings Poor shower arrangement Typical damaged ceilings Existing clinical wash basin clinical floor tiling Defective AHU to Recreation Existing departmental signage Damaged toilet fittings Incomplete theatre ceiling Existing poor furniture Cracked lighting diffusers Poor and missing clinical skirting Replacement Air Handling Unit Temporary room signage Damaged door leaves Damaged roof Defective roof perimeter Original fitted furniture Split joints, and walls without skirtings Fire Alarm panel – non compliant Poor, steep access ramp Damaged and Defective Fittings Sanitaryware and floor Chipped sanitaryware Damaged and Missing Ceilings Typical existing DX split condensing unit Damaged existing roof fans Existing temporary door signage Existing clinical wash hand basin Missing and water stained tiles Existing clinical flooring Existing emergency lighting Existing defective clinical flooring Missing and water stained tiles Existing defective clinical flooring poor vinyl installation Damaged chilled water pumps Existing departmental defective light fittings Damaged door leaves Existing clinical ceilings Existing floor tiling to toilets Existing poor clinical skirtings Temporary room signage Existing defective furniture Damaged clinical wash hand basin Old style distribution board BUILDING: MH LEVEL 2LOCATION: OPERATING RM. 16PICTURE: STORAGE AREA FOR SURGICAL EQUIPMENTCOMMENTS: TYPICAL HANDLING OF MEDICAL EQUIPMENT AND STORAGE?! BUILDING: O.P.B LEVEL 0LOCATION: LOW CURRENT ROOM NEAR ROYAL KITCHEN PICTURE: BOXES OF OLD OPB PLANCOMMENTS: IMPROPER USAGE/STORAGE OF MATERIALS. IT SHOULD BE PLACE OR STORE IN ENGINEERING DEPT. BUILDING: MH LEVEL 2LOCATION: OPERATING RM. 10PICTURE: STORAGE AREA FOR SURGICAL SUPPLIESCOMMENTS: WHAT A WASTE OF BLDG. OR’s THAT COST AROUND 2.5 TO 4M S.R. AND USED FOR STORAGE! BUILDING: O.P.B LEVEL 0 LOCATION: ELECT. ROOM (NO .B5) PICTURE: EXPOSED SECURITY ACCESS CABLES. COMMENTS: IF NOT USE REMOVED OR ARRANGE PROPERLY. BUILDING: M-H LEVEL 0LOCATION: INSIDE ELEC. ROOM NR. ELECT. RM. B24A PICTURE: TELEPHONE TERMINAL BOARD COMMENTS: TELEPHONE TERMINAL BOARD IS NOT PROPERLY ORGANIZED.
Hospitals are the most complex of building types. Each hospital has a wide range of services and functional units: • clinical laboratories, • imaging, emergency rooms, and surgery; • hospitality functions, such as food service and housekeeping; • inpatient care or bed-related function.
Every owner wants a cost-effective building. But what • does this mean? • Is it the lowest first-cost structure that meets the program? • Is it the building with the longest life span? • Is it the facility in which users are most productive? • Is it the design with the lowest operating and • maintenancecosts? • Is it the building that offers the greatest return on • investment?
Differs from almost all other types of buildings. The biological flora that are endemic to all health premises pose a risk to both patients and staff.
Goals: • Running a hospital building over the course of its useful life. • To achieve the intent of the original building design team. • To achieve long-term goals of economy, energy efficiency, resource conservation, & pollution prevention, while meeting the comfort, health, and safety requirements of Patients, Staff and Visitors.
If we “Cannot Measure it” • we • “Cannot Manage it” The development of meaningful measurement criteria: • Key Performance Indicators (KPI’s) is a vital step in • establishing & improving quality
Environment where Standards and Quality are in alignment. To meet the Goals and Objectives of the Healthcare Organizations mission.
Insight, creates meaning, judgmental, actionable Human, tacit, transfer requires learning Wisdom Knowledge Information Contextual Codifiable, explicit Easily transferable Data
Patient involvement: …they cannot and should not be responsible for their own safety in an environment over which they have no control. George AnnasNEJM 354;19:2063-2066
Appropriate circulation ceilings Appropriate boiler plant installation Appropriate Pump assembly Additional wall outlets Appropriate slip resistant vinyl flooring New air cooled liquid chillers Appropriate slip resistant vinyl flooring Typical new distribution board Flat roof being recovered Flat roof with gravel blast Sheet vinyl to Ward areas Typical fitted furniture Appropriate slip resistant vinyl flooring Appropriate clinical basin and mixer tap Cantilever type fitted furniture New domestic wc and cistern Panel mounted clinical wash hand basin Corridor suspended ceilings Proposed new split DX units Appropriate room signage Appropriate laminated doorsets Appropriate clinical toilet arrangement Appropriate slip resistant vinyl flooring Appropriate type fan fittings washable clinical ceiling Proposed fitted clinical furniture Compliant Fire Alarm panel New Designed steam boiler
High-level Blueprint for Healthcare System Governmental Control and Oversight • Supervision and Consultation • Legislative Authority Regulations for Private Investment Competition, and Pricing Regulations Accreditation and Quality Control Healthcare Funding / Health Insurance Compensation of Providers • Antitrust Laws and Regulations • Pricing Regulations • Regulations on Choice of Professional Activity • Sources of Funding • Requirements for Insurance Coverage • Tasks and obligations of Insurers • Sources of Funds • Rules for Compensation • Rules for and Protection of Private Investments • Rules for and Protection of Foreign Investments and Property • Provider Institutions • Pharmaceuticals • Medical Products Source: Booz Allen analysis
Government-Driven Health-Related Initiatives Cooperative Health Insurance Act • Regulates the provision of healthcare for non-Saudi residents in the Kingdom • Determines the rights and duties of sponsors, beneficiaries, insurers and providers Saudi Food and Drug Administration • Responsibility for regulating activities related to the safety of food and drug for man and animal, and the safety of biological and chemical substance, as well as medical devices Nat. Center for Health Insurance Standards • Establish national standards, unify health industry processes, and play an advocacy and educational (training) role in developing an advanced healthcare delivery system Saudi Council for Health Specialties • Develop the professional practice, promote technical skills, enrich scientific thought, and promote practical applications related to health specialties Private Health Institutions Legislation • Set rules and guidelines that govern the set up and operation of private health institutions, including infrastructure, human resources, medical services, etc. Makkah Region Quality Program • Establish quality standards for public and private sector hospitals and other care delivery institutions – activities limited to Makkah region Source: Booz Allen analysis
Accreditation Auditing Standards Quality System
Auditing Standards Quality System