Download
1 / 8
130 likes | 465 Vues
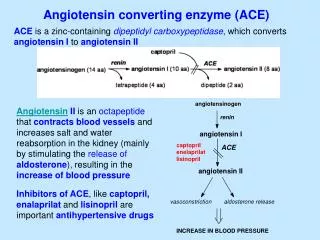
PEACE Trial. Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) Trial. Presented at The American Heart Association Scientific Sessions 2004 Presented by Dr. M. Pheffer. PEACE Trial. 8,290 patients with stable coronary artery disease without heart failure

E N D
PEACE Trial Prevention of Events with Angiotensin Converting Enzyme Inhibition (PEACE) Trial Presented at The American Heart Association Scientific Sessions 2004 Presented by Dr. M. Pheffer
PEACE Trial 8,290 patients with stable coronary artery disease without heart failure MI, CABG, or PCI at least 3 mo prior to enrollment, normal LV wall motion w/ EF>40% 82% male, mean age 64 years 90% received Aspirin, 60% beta-blockers, 70% lipid-lowering therapy ACE Inhibitor Trandolapril 4mg/day At 1 year, Trandolapril or open-label ACE inhibitor taken by 81.9% At 3 years, 74.5% n=4,158 • Placebo • At 1 year, 1.5% of patients on Ace inhibitor • At 3 years, 8.3% • n=4,132 • Primary Endpoint: • Composite of cardiac death, MI, or revascularization at a mean follow-up of 4.8 years Presented at AHA 2004
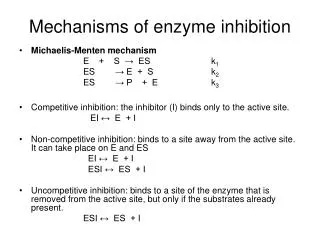
PEACE Trial: Primary endpoint Primary Composite of cardiovascular death, nonfatal MI, and coronary revascularization p = 0.43 • The primary composite endpoint of cardiovascular death, MI, and revascularization was equal between the Trandolapril and Placebo groups at a mean follow-up of 4.8 years • The primary endpoint was also equivalent in all analyzed subgroups Presented at AHA 2004
PEACE Trial: Primary Endpoint The individual components of the primary endpoint were also equivalent in the Trandolapril and placebo groups p=0.65 p=0.24 p=1.00 p=0.67 % Presented at AHA 2004
PEACE Trial: All Death All-Cause Death p = 0.13 • A slight reduction in all-cause death seen in the Trandolapril arm was not statistically significant Presented at AHA 2004
PEACE Trial CHF as the primary cause of hospitalization or death and new-onset diabetes were both significantly lower in the trandolapril group. Neither analysis was a primary or secondary endpoint. New onset diabetes p = 0.01 CHF as primary cause of hospitalization or death p = 0.02 % % Presented at AHA 2004
PEACE Trial: Safety Side effects leading to discontinuation p < 0.001 • There was a significantly higher incidence of side effects leading to drug discontinuation in the Trandolapril group. • The Trandolapril group also had significant increases in cough and syncope Presented at AHA 2004
PEACE Trial: Summary • Among patients with stable coronary artery disease and no heart failure, there was no difference in the primary composite endpoint of cardiovascular death, nonfatal MI, and coronary revascularization with the ACE inhibitor trandolapril or placebo. • All individual components of the primary endpoint were equivalent between the two groups. • A retrospective analysis of new onset diabetes and CHF as the primary cause of hospitalization or death was found both to be lower in the trandolapril group. • Trandolapril was associated with a significantly higher incidence of side effects leading to drug discontinuation. Additionally, cough and syncope were each significantly higher in the trandolapril cohort. • The lack of benefit from ACE inhibitor therapy seen in this trial differs from the results of several previous trials including the HOPE and EUROPA trials, which showed significantly lower incidences of cardiovascular death, MI, stroke, and cardiac arrest in patients treated with ACE inhibitors than in those treated with placebo. • A possible reason for the lack of benefit with trandolapril could be that most patients were more aggressively managed for risk factors with lipid-lowering medication and previous revascularization. In accordance with this hypothesis, the PEACE trial had a lower event rate than the EUROPA and HOPE trials.