Download
1 / 18
180 likes | 382 Vues
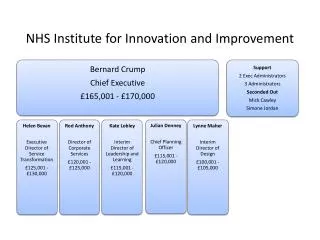
Board Integrated Performance Report 25 th July 2019 June 2019 Data. 1.3 NHS Improvement Finance Score. 1.2 NHS Improvement Segment. 1.1 CQC Rating. Requires Improvement. 2. 3. Workforce – Sickness Absence.

E N D
Board Integrated Performance Report 25th July 2019 June 2019 Data 1.3 NHS Improvement Finance Score 1.2 NHS Improvement Segment 1.1 CQC Rating Requires Improvement 2 3
Workforce – Sickness Absence • The in-month sickness rate for June 2019 has reduced by 2.3% to 4.5% from a high in January 2019 of 6.8%; an average monthly financial gain of £185k. Further analysis of data in that period shows: • the reduction is due mainly to fewer long term absences (5% to 3.3%); a net 15 fewer (86 to 71) in June 2019. • This includes 21 long term cases resolved since January (7 leavers / 16 returned to work). • The number of overall episodes reduced in that period from 627 to 308. • Sickness days reduced from 5,461 to 3,475 days, or £492k to £307k p/m. • Anxiety, Stress, Depression and Musculo-skeletal remain top reasons for long term sickness.
Workforce – Labour Turnover (LTO) There were 351.68 WTE leavers in the last 12 months. Although labour turnover has increased in the last four months, SPC analysis indicates this is natural variation (5 data point) not a rising trend (6 or more data points). Notably, the Trust’s internal turnover target is below the lower control limit. The target is therefore not forecast to be met under the current processes. Labour turnover remains a challenge for most NHS organisations and NHS Improvement recently fed back to the Trust that we are one of the top performers in this area. Bradford 0-19 Tender Impacts on LTO: if LTO was re-stated to discount required turnover (managed across Wakefield & Bradford) to manage within the Bradford 0-19 contract the June LTO would be around 11.6%. The chart will be reviewed to draw out key changes. Key reasons for leaving have remained static for the last few years, being: retirement; relocation; work-life balance; promotion. The variation by service table also highlights the significant positive net increase in overall Mental Health Care Group staff e.g. EIP, acute recruitment and new Care Closer to Home staff.
Workforce – Mandatory and Required Training Exceptions: Actions: The key current area of focus is to secure rapid improvement in rates of CPA and Mental Health Act compliance. Trajectories are being established for all under-performing teams for both requirements. The training lead is mapping current and considering the need for any additional capacity. Daily Lean Management will be used to monitor and ensure rapid progress. Compliance rates and exceptions have been shared with the training lead to ensure tailored improvement plans can be matched with available and required capacity. Progress will be reported in the September Board Integrated Performance Report and tracked by the Senior Leadership Team in the interim.
Workforce – Appraisal Rates Performance remains generally strong and 9.8% above appraisal levels as at June 2018. Exceptions: Whilst Bradford 0-19 Service records show the highest number of appraisals recorded as out of date (at 70.8% a total of 71 out of date), further review indicates that this included a number of leavers, staff on long-term absence or secondment to other services. Records are being corrected and appraisals booked where out of date. Actions: For individual service or corporate teams which are currently below the target of 80%, the Head of HR and HR Business partners are contacting managers and team leaders directly to review their compliance and ensure that appraisals are booked in and / or ESR updated to reflect.
There were 2 new reported serious incidents in June: 1 suspected suicide of a service user on leave from Airedale Centre for Mental Health and a suspected suicide of a service user under Child and Adolescent Mental Health Services (CAMHS). Serious incidents are monitored in the weekly Quality and Governance call out meeting and have been included in the Quality & Safety Committee dashboard and reported every six weeks. • 11 investigations are ongoing and 3 investigations have exceeded the 12 week timescales to complete and have required extensions: • A Panel-led investigation into an Inpatient suspected suicide has been extended due to the complexity of the investigation and number of staff needing to be interviewed. • The HR Lead Investigator in a joint HR/Serious Incident investigation has been waiting for a critical meeting with the service user however the previously planned meeting had been cancelled by the Service User. The report is now due to complete w/c 15th July 2019. • Community Mental Health Team – Suspected suicide. A query relating to the administration of medication was identified towards the end of the investigation. As a result a meeting with the Lead Pharmacist was necessary – now complete. The report is complete and has been circulated for comment prior to presentation to the Serious Incident Approval panel.
Compliments, Complaints and Concerns over the 24 months July 2017 to June 2019 Complaints Exception: There has been an increase in the number of formal complaints. This is across a range of services, however the majority have been linked to Community Mental Health Teams. These have been reviewed and whilst some relate to discharge from services including changes relating to the functional medical model. There were no themes or trends with regard to staff involved. Of 2 cases relating to Palliative Care services both concerns were about nursing care delivered. Complaints and concerns are monitored through the weekly Quality Governance call out meeting, and monthly data is provided to the monthly SLT dashboard, with reporting into Quality and Safety Committee dashboard every six weeks. Compliments Highlight: District Nursing and First Response services received the highest reported compliments with positive comments about the level of support both teams had offered to service users and carers.
Exception: The apparently significant increase in pressure ulcers reported in May 2019 reflects in part delays in teams managing their reports, with pressure ulcers then counted in the subsequent month. • Actions to ensure responsive reporting and action: Delays in report management have been addressed by the service manager. From 1 May teams were asked to start reporting moisture lesions to enable identification of care homes that may need additional training. May 2019 data includes 43 moisture lesions. • Actions taken in management of pressure ulcers: • The tissue viability team have completed 35 bespoke training sessions to all district nursing teams and community matrons, resulting in 98.8% training compliance. Pressure ulcer prevention training is undertaken for all new staff upon induction. • The tissue viability team are exploring options of collating pressure ulcer data in a more meaningful way, for example in comparison with caseload sizes. • A deep dive is being undertaken and a full update will be provided to the August 2019 Quality & Safety Committee. Progress to date includes: • Data has been collated and under review, including demographics of the area, team structure and risks; • Actions identified including: caseload cleanse; review of appraisals (all are now in date); review of training needs with all staff received or booked onto relevant training; review of caseload/areas – one care home temporarily transferred to another team; review of store rooms and processes complete and system in place for managing stock; staff supported to fully engage with SystmOne tasks, referrals and triage; monthly team meetings commenced; work taking place on safety huddles.
Mental Health Legislation Committee Integrated Performance Report - Meeting 18th July 2019. Data up to 30th June 2019 Lead Director: Patrick Scott, Chief Operating Officer. Sections Reviewed on time: This metric examines whether the care team and in particular the Responsible Clinician (RC) have reviewed whether continued detention under the MHA is still required at a point in time ahead of that section’s expiry date. Where breaches occur, this is usually with a patient detained under Section 2 (which is valid for 28 days) who has not had their detention reviewed (or the RC has decided for clinical reasons to allow the maximum period of detention to be used) before making a next step care plan. Error-free Sections: This metric examines the percentage of sections that passed necessary levels of scrutiny, were regarded as error-free and therefore a lawful detention. Exceptions: The new stretch target of 98% was breached in April for both measures. Section 2 Lapses: There were 4 lapses in April: A RC had allowed two sections to lapse due to diary errors but renewed the next day; One lapsed because the patient was absent without leave and the care team decided not to extend the Section 2; One lapsed because the Nearest Relative order for discharge occurred towards the end of the Section 2 and the RC decided not to seek a renewal. Cancelled Sections: 3 sections were cancelled in April: The nurse did not accept the papers for One Section 5(2); One Section 2 was cancelled because the AMHP had not signed the report; One Section 3 was cancelled because page 3 of the application was unsigned.
Single Oversight Framework Operational Performance Metrics Maximum time of 18 weeks from point of referral to treatment (RTT) in aggregate − patients on an incomplete pathway Community Dental Service (CDS) National benchmark figure 86.9% as of May-19: next publication date 08/08/19 Exception: June 2019 Performance is below the 92% target for patients who require dental treatment under general anaesthetic. The SPC chart shows this is a single point below the lower control limit and therefore special cause variation (changes in the data that are unexpected). However performance usually decreases in the first quarter of the financial year as dental theatre sessions (held on Mondays and Fridays) are impacted by the Easter and two May bank holidays. Due to the timing of Easter, there were 3 bank holiday days in April and May 2018 (3 of 17 planned sessions; 17.6%) but there were 4 bank holiday days (4 of 18 planned sessions; 22.2%) in the same period in 2019; a 4.6% loss in capacity compared to the same period in 2018. The increased waiting times relate to paediatric special care, where patient complexity has increased and in which there has been a 30% increase in list size over the last 3 years. There is no additional theatre capacity at Bradford Royal Infirmary or Airedale General Hospital. The CDS closely manage processes for treatment under general anaesthetic, with weekly reviews of any patient wait over 15 weeks. Additional actions include a review with the paediatric team of the criteria for treatment under general anaesthetic to consider alternative treatment and require consultant/specialist opinion before accepting any child for treatment under general anaesthetic. Following validation of the waiting list in mid July, a trajectory for achievement of the 18-week waiting time standard will be agreed. The national benchmark figure relates to total referral to treatment performance. Local intelligence is that no other Community Dental Service in Yorkshire and Humber is currently meeting the 18-week target.
Single Oversight Framework Operational Performance Metrics Improving access to psychological therapies (IAPT): Proportion of people completing treatment who move to recovery (from IAPT minimum dataset) Early Intervention in Psychosis: People with a first episode of psychosis begin treatment with a NICE-recommended package of care within 2 weeks of referral National Benchmark 52.9% as of Apr-19: next publication date 08/08/19 Recovery rate at overall Trust level was 58% in April (final published data) reducing to 50% in May (initial data). SPC analysis shows that this is natural variation. The recovery rate target was met for Bradford Districts and Airedale, Wharfedale and Craven Clinical Commissioning Group (CCG) populations in February, March and April but remains below the 50% target for Bradford City CCG (February 46%, March 44%, April 42%). A proposal for IAPT has been submitted for City CCG via the RICS mental health arrangements. The number of completed pathways in June was 36; 29 of these clients were seen within two weeks. The number of incomplete pathways (patients waiting) at the end of June was 27; 11 of these patients have been waiting for more than two weeks. As a result of new staff in place and scheduling of additional assessment slots to assess the expected numbers of referrals, performance improved from November 2018. SPC analysis shows that this is an improvement that would not result from natural variation in the system.
Single Oversight Framework Operational Performance Metrics Indicator M22: The Data Quality Maturity Index (DQMI) mental health services dataset score (MHSDS) data score is a quarterly publication from NHS Digital. There are 361 data items within the MHSDS. NHS Digital introduced 11 new data items to the DQMI data score, applied retrospectively from December 2018 data. The number of indicators will gradually increase to 31 measures as part of the national 2019/20 commissioning for quality and innovation indicator, applicable from 2019/20 quarter 3. Work is taking place to identify system configuration changes to ensure the clinical system is capable of recording necessary data items, following which work will be needed by operational services to improve collection of any data item under-performing.
Contracts – Quality Performance Indicators and Commissioning for Quality and Innovation (CQUIN)