Download

1 / 38
390 likes | 672 Vues
Renal Replacement Therapy. Optimal Pre-ESRD Management. Preventing or slowing progression Preventing complications of uremia such as anemia, ROD & malnutrition Preparing the patient for the RRT Planning for the creation of a permanent access for hemodialysis

E N D
Optimal Pre-ESRD Management • Preventing or slowing progression • Preventing complications of uremia such as anemia, ROD & malnutrition • Preparing the patient for the RRT • Planning for the creation of a permanent access for hemodialysis • Planning for hemodialysis initiation before major symptoms of uremia arise
Renal Replacement Therapy • Dialysis • Hemodialysis • In-center • Home • Peritoneal dialysis • IPD • CAPD • Cycler dialysis • Transplantation
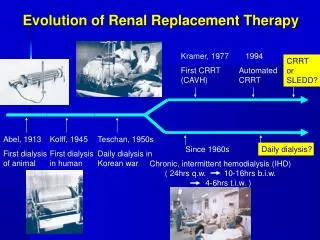
History • Dialysis is a Greek word meaning "loosening from something else". • Dialysis is referred to as "selective diffusion." Diffusion is the movement of material from higher concentration to lower concentration through a given membrane • Thomas Graham, Chairman of Chemistry at University College, London, first discovered this idea of selective diffusion
Dialysate • A chemical bath used in dialysis to draw fluids and toxins out of the bloodstream and supply electrolytes and other chemicals to the bloodstream.
AVF Creation in CRF • Cr clearance < 25 ml/min • Serum Cr > 4 mg/dl • Within 1 year of the anticipated need for maintenance dialysis therapy
Starting HD IN CRF • HD should be initiated at a level of residual renal function above which the major symptoms of uremia usually supervene: • 9 < Cr cl < 14 ml/min • It may be necessary to initiate patients even earlier in their course if they have otherwise uncorrectable symptoms or signs of renal failure
Hemodialysis Treatment Progress in Therapy and Technology Increases Quality of Life for the Patients
Initiation of dialysis in patients with ARF • Refractory fluid overload • Hyperkalemia (plasma potassium concentration >6.5 meq/L) or rapidly rising potassium levels • Metabolic acidosis (pH < 7.1) • Azotemia (BUN > 80 to 100 mg/ dl)
Initiation of dialysis in patients with ARF 5.Signs of uremia, such as pericarditis, or an otherwise unexplained decline in mental status 6.Severe dysnatremias (155 < Na < 120 meq/L) 7. Hyperthermia 8. Overdose with a dialyzable drug/toxin
Indications For Heparin-Free dialysis • Pericaditis • Recent surgery, with bleeding complications or risk. Especially: • Vascular & cardiac surgery (within 7 days) • Eye surgery (retinal & cataract) • Renal transplant • Brain surgery (within 14 days)
Indications For Heparin-Free dialysis • Coagulopathy • Thrombocytopenia • ICH • Active bleeding • Routine use for dialysis of acutely ill patients by many centers
In Hospital Management of Patients with CRF & ESRF • Diet regimen • Prevention of ARF • Restriction of blood sampling • Restriction of blood transfusion • Treatment of uremic bleeding defects • Dose adjustments of drugs • Pre-operation dialysis
Risk Factors of ARF • Renal Hypoperfusion • Preexisting Azotemia • Sepsis • Nephrotoxins • Electrolyte Disorders
Treatment of uremic bleeding defects • Dialysis • DDAVP 0.3 μg/kg IV 3 μg/kg IN • Cryoprecipitate • RBC Transfusion • Conjugated estrogens • FFP
Renal Transplantation • Cadaveric Donor • Living Donor • Non related • Related • Spouse
Exclusionary Conditions for Renal Transplantation • Patient will not live more than 1 year • Metastatic malignancy, not responsive to therapy • Acute or chronic infections that are not controlled • Severe psychiatric disease that impairs patient's consent & compliance • Medical incompliance • Substance abuse • Immunologic incompatibilities
Criteria That Exclude a live Donor • Age < 18 • Severe HTN • DM • Hx of nephrolithiasis • Impaired renal function • Morbid obesity • Strong family history of DM • FHx of hereditary nephritis or polycystic kidney disease • Hypercoagulability • HIV, HB, HC infection • Uncontrolled psychiatric disorders
Drugs Used in Maintenance Immunosuppression • Calcineurin Inhibitors • Cyclosporine • Tacrolimus • Azathioprine • Mycophenolate Mofetil • Glucocorticoids
In Hospital Management of Renal Transplant Patients • Diet regimen • Prevention of ARF • Restriction of blood sampling • Restriction of blood transfusion • Drugs interactions • Secondary adrenal insufficiency • Prevention of infection • Transplant drugs usage
HD in ARF CAN DIALYSIS DELAY RECOVERY OF RENAL FUNCTION? • There is at least theoretical concern that dialysis might have detrimental effects on renal function. Three factors may be important in this regard: • a reduction in urine output • induction of hypotension • complement activation resulting from a blood-dialysis membrane interaction.
Dry Weight • The lowest weight a patient can tolerate without the development of signs or symptoms of intravascular hypovolemia.
Dry Weight • Estimating dry Weight: Liters of actual body water = 142 × liters of NTBW = 142 × (60% × 60) = 38.72 Predialysis serum Na 132 38.72 – 36 = 2.72 lit NTBW= Normal Total Body Water