Download
1 / 55
600 likes | 1.12k Vues
Stomach & Barium Meal . RT-205B MIDTERM. What is a stomach?. Stomach. A dilated, saclike portion of the digestive tract extending between the esophagus and the small intestine. Serves as the reservoir for swallowed food and fluid. It has an entrance valve and exit valve of food materials

E N D
Stomach & Barium Meal RT-205B MIDTERM
Stomach • Adilated, saclike portion of the digestive tract extending between the esophagus and the small intestine. • Serves as the reservoir for swallowed food and fluid. • It has an entrance valve and exit valve of food materials • Esophageal Sphincter • Pyloric Sphincter
The stomach is about 12 inches (30.5 cm) long and is 6 inches. (15.2 cm) wide at its widest point. The stomach's capacity is about 1 qt (0.94 liters) in an adult.
4 – layers of stomach • Covering layer, the serosa • Muscular layer consisting of oblique, circular, and longitudinal fibers • Sub-mucus layer • Thick, soft mucosal lining(rugae)
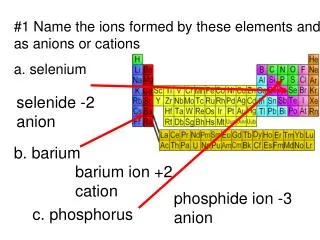
4 – division of stomach • Cardia • Fundus • Body • Pyloric portion
Parts of the Stomach • Cardia • is the section immediately surrounding the esophageal opening. • Fundus • is the superior portion of the stomach that expands superiorly and fills the dome of the left diaphragm. • Body • descending from the fundus and beginning at the level of the cardiac notch. • Pyloric portion • distal part of the stomach. • Consist of the – pyloric vestibule and pyloric antrum.
Barium Meal/Upper GI series • Radiographic examination of the distal esophagus, stomach, and duodenum with the use of radiolucent and radiopaque contrast medium.
Function • To study radiographically the form and function of the distal esophagus, stomach, and duodenum, as well as to detect abnormal anatomical and functional conditions.
Indications • Peptic ulcer • Hiatal hernia • Acute or chronic gastritis • Tumor, carcinoma and benign • Diverticulum • Bezoars
Clinical Indication • Peptic Ulcer - Erosions of the stomach or duodenal mucosa due to various physiological or environmental conditions, such as excessive gastric secretions, stress, diet and smoking.
Clinical Indications • Hiatal Hernia • portion of stomach will herniate through the diaphragmatic opening. • Gastritis • Inflammation of the lining or mucosa of the stomach. • Tumor • Small mass growing from the mucosal wall.
Clinical Indications • Diverticula • are a weakening and out-pouching of a portion of the mucosal wall. • Bezoar • mass of undigested material that gets trapped in stomach.
Contraindications: • Patient has a history of bowel perforation, laceration, or viscous rupture, the use of barium sulfate may be contraindicated. • Complete large bowel obstruction
If suspected for perforation • For the assessment of the site of perforation it is essential that a water-soluble contrast media is used (ex. LOCM or Non-ionic contrast media)
Patient Preparation: • Soft, low-residue diet for 2 days(to prevent gas formation) • The day before – patient should be NPO or cleansing enemas may be given to assure a properly clean colon. • Food and fluids should be withheld for at least 8 to 9 hours prior to examination. • Patient is not allowed to smoke cigarettes or chew gum during NPO period. • To x-ray department for examination
2 – General GI – examination Technique are used • single contrast method • double contrast method
2 – General GI – examination Technique are used • Double contrast – the method of choice to demonstrate mucosal pattern. • Single contrast – uses; • Children – since it usually is not necessary to demonstrate mucosal pattern • Very ill adults – to demonstrate gross pathology only.
Different type of Examination of the GI tract • Biphasic examination • combination of single and double contrast. • Hypotonic Duodenography • requiring intubation • used for evaluation of postbulbar duodenal lesions and for the detection of pancreatic disease. • Described by Liotta.
Position of Patient: Stomach • RAO – to demonstrate the antrumand greater curve • SUPINE – to demonstrate the antrum and body • LAO – to demonstrate the lesser curve en face • Left lateral tilted, head up 450 – to demonstrate the fundus
Cont… • From the left lateral position the patient returns to supine position and rolls into his left side and over into a prone position. • This sequence of movement is required to avoid barium from flooding into the duodenal loop. • Duodenal loop • Prone – patient is lies on a compression pad to prevent barium from flooding into duodenum • RAO – additional view of anterior wall of the duodenal loop
Spot films of the duodenal cap • Prone • RAO – the patient attains the is position from the prone position by rolling first onto the left side, for the reasons mentioned. • Supine • LAO
Additional views • Erect position – demonstrate the fundus if there are suspected lesions. • Spot film of the esophagus are taken, while barium is being swallowed, to complete the examination.
Position of Patient: Stomach • Upright PA projection (14x17) • To demonstrate the type and relative pos. of the stomach. • Upright left lateral position • Demonstrate the left retrogastric space • Recumbent PA projection • demonstrate gastroduodenal surfaces • CR angled 20 – 25degs cephalic – infants • 35 – 45degs cephalic - adults
Cont… • One or more Recumbent RAO positions • gastric peristalsis is usually more active in this position. • A right lateral position is used to demonstrate the duodenal loop in profile, duodenojejunal junction, & right retrogastricspace. • Recumbent AP projections, • 11x14 films demonstrate the retrogastric portion of the duodenum and jejunum.
Modification of technique for young children • The examination is modified to identify the three major causes of vomiting – gastro-esophageal reflux, and pyloric obstruction. • Single contrast technique is used with 100% barium and no paralytic agent. • Small volume of barium – enough to just fill the fundus in a supine position • Child is in semi prone into a LPO or RAO. A better advantage if 20-400caudal.
Cont… • Once barium enters the duodenum, the infant is returned to supine position and a radiograph is taken with child supine perfectly still as barium passes around the duodeojejunal flexure. • Once malrotation is diagnosed or excluded, a further volume of barium is administered until the stomach is reasonably full. • The child is rotated 180 to elicit gastro-esophageal reflux
After Care • Patient is advised to drink lots of water and expect to have a white fecal. • Laxative should be taken to totally remove the barium to avoid barium impactions, which is painful
Complications • Leakage of barium from an unsuspected perforation • Aspiration • Conversion of partial large bowel obstruction to a complete obstruction by impaction of barium
Small Intestine • Small Bowel Series • Radiographic study specifically of the small intestine. • Purpose: • to study the form and function of the 3 – components of the small bowel, as well as to detect any abnormal conditions.
Clinical Indication • Enteritis or gastroenteritis • Neoplasm • Malabsorption syndromes • Ileus
Cont… • Enteritis • term describing the inflammation or infection of the small bowel. • Neoplasm • describing “new growth”. • This new growth may be benign or malignant. • Malabsorption Syndromes • GI tract is unable to process and absorb certain nutrients. • Sbs – mucosa may appear to be swollen or thickened due to the content irritation. • Ileus • obstruction of the small intestine.
2 – types of Ileus • Adynamic or Paralytic • due to the cessation of peristalsis • Mechanical obstruction • physical blockage of the bowel. • (ex. tumor, adhesions, or hernias)
2 – strict contraindications • Pre-surgical patients & suspected a perforated hollow viscous. • Possible large bowel obstruction.
Procedures: • 4 – methods • UGI – Small bowel combination • Small bowel series • Enteroclysis • Intubation method
UGI – Small bowel combination • Basic Routine: • routine UGI – Series • note time patient ingested 1st cup(8 oz) of barium. • Ingested 2nd cup of barium • 30 min. PA – radiograph • ½ hour interval radiographs( iliac crest – center) • until barium reaches large bowel (usually 2 hrs.) • 1 hr. interval radiographs, if more time is needed after 2 hours
Small Bowel Series • Basic Routine: • plain abdomen radiograph (scout) • 2 cups (16 oz) of barium ingested ( note time) • 15 – 30 min. radiograph • ½ hour interval radiographs until barium reaches large bowel (2hrs) • 1 hour interval radiographs, if more time is needed.
Enteroclysis – SBS • Basic Routine: • Thru the nose, an intubation into the duodenum • barium sulfate suspension is instilled • air or methylcellulose is instilled • fluoroscopic spot films & conventional radiographs are taken. • Upon successful completion of exam, intubation tube is removed.
Intubation method – SBS • Basic Routine: • A tube inserted in the mouth until to the duodenum • contrast media instilled • note time that contrast media is instilled • 15 – 30 min. radiographs • radiologist will specify filming sequence after 2 hrs.