Download
1 / 43
430 likes | 906 Vues
Thoracic Aorta Trauma. Charles E. Smith, MD Professor of Anesthesia Director, Cardiothoracic Anesthesia MetroHealth Medical Center Case Western Reserve University Cleveland, Ohio April, 2005. Objectives. Incidence Pathophysiology Diagnosis Anesthetic management

E N D
Thoracic Aorta Trauma Charles E. Smith, MD Professor of Anesthesia Director, Cardiothoracic Anesthesia MetroHealth Medical Center Case Western Reserve University Cleveland, Ohio April, 2005
Objectives • Incidence • Pathophysiology • Diagnosis • Anesthetic management • Preop evaluation, monitoring • Anesthetic agents • Neuroprotection • One-lung ventilation
Incidence • 12- 30 % blunt trauma deaths • 8000 deaths/yr, USA • 2nd most common cause of death in 1 study (after head injury) • Majority (80-85%) die at scene • Etiology: MVAs, falls, crush, pedestrian struck, airplane crash Smith: Am J Surg 1986;152:660
Mechanism of Injury Fabian et al: J Trauma 1997;42:374-80
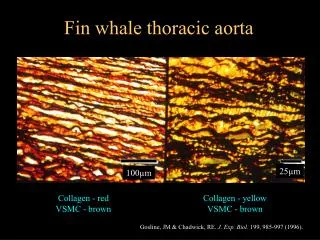
Pathophysiology • Survivors have intact adventitia • Hematoma contained by parietal pleura + surrounding tissue: “false aneurysm” • Most common injury near ligamentum arteriosum, distal to left subclavian (prox descending): 65-93% • Other sites of injury: • Ascending / Arch: 7-14% • Mid or Distal Descending: 4-12% • Multiple Sites: 4-13% Wall MJ et al: Surg Clin N Am 2001;81(6):22. Fabian: J Trauma 1997;42:374
Diagnosis • Abnormal mediastinum on CXR: • predominant initial finding in 85%; good screening tool • Spiral Chest CT: • high negative predictive value • useful as screening + diagnosis • Aortography: gold standard at MHMC • TEE: sensitive + specific; also useful for BCI • may not be as available as CT or angio • may miss ascending /arch injuries + branches EAST: www.east.org; Vignon et al: Anesthesiology 2001;94:615-22
Anesthetic Management • Depends on location + extent of injury • Ascending / Arch: • requires CPB + possible circulatory arrest • Descending- clamp + sew vs. distal perfusion • Timing of surgery- delayed vs. emergent repair • Endovascular stent-graft repair: feasible in some centers, but still risk paraplegia, death... Criado et al: J Vasc Surg 2002;36:1121-8
Blunt Chest Trauma: Extra-thoracic Injuries Besson + Saegesser 1983; Switzerland, N= 1485 chest injuries
Management Besson, 1983
Delayed Repair • Historically- 1% mortality per “unoperated” hr • 1981: 14/44 had repair 2-79 days after injury, no rupture while waiting [Akins] • 1989: 15/21 had repair after 4 wks, no rupture while waiting [Blegvad] • 1991: case of spont healing of tear [Wigle] • 1995: 82% survival w delayed repair, 1 day- 7 mos • 1997: 86% survival if “elective” thoracotomy [Fabian]
Delayed Repair @ MHMC Kwon, Gill IS et al: Ann Thorac Surg 2002;74:S1888-91, N=57, ISS 31-40. 60% distal perfusion, 40% clamp + sew
Blunt Cardiac Injury (Myocardial Contusion) • Spectrum of problems • enzyme abnormalities, ST segment • arrhythmias: PVCs, RBBB, VT • wall motion abnormalities • cardiac failure • cardiac rupture • Dx: ECG, echo www.trauma.org/thoracic/index.html
Risk of Surgery with BCI: No Deaths, but... Flancbaum L: J Trauma 1986;26:795; Ross P: Arch Surg 1989;124:506
Monitoring • Standard + invasive monitoring • Art line: • left radial or fem if ascending or arch tear • right radial or fem if proximal descending tear • provides beat to beat BP • only way to measure BP if full CPB • facilitates blood sampling • Pulmonary artery catheter (PAC)
Pulse Contour Analysis • Sensitive method of predicting SV or CO in response to volume after cardiac surgery and in ICU [Reuter DA: BJA 2002; 88: 124; Michard F: Chest 2002; 121: 2000 ] • Similar estimates of preload v. echo during graded hemorrhage in animals [Preisman S: BJA 2002; 88: 716] • Helpful tool in dx of hypovolemia after blast injury [Weiss YG J Clin Anesth 1999; 11: 132
Systolic Pressure Variation • Difference between maximal + minimal values of systolic BP during PPV • down: ~ 5 mm Hg due to venous return • up: ~ 5 mm Hg due to inspiratory in LV output • SPV > 15 mm Hg, or down > 15 mm Hg: • highly predictive of hypovolemia Marik: Anaesth Intensive Care 1993;21:405. Coriat: Anesth Analg 1994;78:46
IJ Cannulation + Ultrasound • View anatomy in real time • Visualize desired target vessel + note location, size, patency • Identify abnormal anatomy • Eliminate difficult sticks • complications Sulek CA: www.scahq.org/sca3/newsletters/2002oct/pro.shtml
PAC Indications: ASA Task Force • High risk patient with severe underlying cardiopulmonary disease • Intended surgery places patient at risk because of magnitude or extent of operation • Practice setting suitable for PAC monitoring: OR, ICU, nursing www.asahq.org/publicationsandservices/pulm_artery.pdf
Anesthetic Agents • Medical control of BP • β- blockers / Vasodilators: esmolol, labetalol, metoprolol / NTG or SNP • Extreme importance if delayed surgery • Induction + maintenance: many combinations have been used safely: • lidocaine, etomidate, fentanyl, roc / vec, • low dose isoflurane, avoid N2O • Inotropes + vasopressors: • major hemodynamic alterations after unclamping / CPB • cardiac dysfunction from multiple causes
Dexmedetomidine: α-2 Agonist • Advantages: • HR +BP, attenuation of stress response • Analgesia + sedation, minimal respiratory depression • Disadvantages: • transient hypertension if loading dose • hypotension + bradycardia • ability to compensate for hypovolemia • Start before AXC [descending surgery] • Start after sternal closure [full CPB] www.scahq.org
Hyperglycemia • neuro injury after focal + global ischemia • Enhanced apoptosis • WBC function • Impaired wound healing • risk infection • Tight control infection and improved outcome • Requires insulin infusion + frequent BS monitoring to POD 3-5 www.starwood.com/research/insulin.html; N Engl J Med 2001;345:1359-67
Van Den Berge Study • RCT, 1548 diabetic + non-diabetic SICU patients • 60% had cardiac surgery • Compared tight vs. conventional glucose control • Tight: 80-110 mg/dl • Conventional: insulin only if glucose > 210; endpoint 180-200 • mortality in tight group 4.6 v. 8% • infections, dialysis dependent RF, # transfusions required, need for prolonged mechanical ventilation N Engl J Med 2001;345:1359-67; CCM 2003;31(2)
Distal Perfusion: Descending • Advantages • Control of proximal HTN • visceral + renal ischemia • acidosis + declamping shock • Easier to rewarm • Access for rapid volume expansion • paraplegia if prolonged AXC O'Connor: J Cardiothorac Vasc Anesth 1995;9:734
Distal Perfusion: Descending • Disadvantages: • Atrial, ventricular, aortic, or femoral artery injury • Air emboli / embolic stroke • Interference with operative field • operative time • Cerberal hemorrhage [15% in 1 study] • Bleeding from cannulation sites • Shunt dislodgement • Difficult exposure for proximal cannulation O'Connor: J Cardiothorac Vasc Anesth 1995;9:734. Anesth Analg 2003;96SCA1-141 [Abstract]
Neuroprotection: Ascending / Arch • DHCA, 19-21 oC + thiopental, 3-5 mg/kg • Pack head in ice + cool additional 5 min after isoelectric EEG [BIS] • Alpha-stat pH management • Slow rewarming • Normoglycemia • Steroids ? Oliver et al: Thoracic Aortic Disease, Ch 24 in Kaplan, Cardiac Anesthesia, 4rth Ed, 1999
Advantages of DHCA • Provides optimal surgical field: • bloodless, quiet, unobstructed • Provides maximal organ protection: • cellular metabolism • excitatory neurotransmitter release • generation of free radicals • consumption of free radical scavengers • permeability of cell membranes • post-ischemic cerebral edema
Disadvantages of DHCA • Limit of “safe” circulatory arrest time: • 40-50 min • Neurologic dysfunction + stroke • Cardiac dysfunction • Metabolic deregulation • Altered cell membrane integrity • Hemorrhagic complications
Neuroprotection: Descending • Descending: (spinal cord) • Mild hypothermia, 35 oC • Normoglycemia • Clamp + sew, clamp time < 30 min • Distal perfusion • Maintain BP at baseline + 1/2 peak XC BP MHMC Descending Thoracic Aorta Protocol
Neuroprotection: Descending • CSF Drainage • SCPP = MAP - CSFp • CSFp monitoring- not routinely done b/c of risks + doubtful benefit w short AXC • BP Control • Maintain higher BP during AXC (v. baseline) • Ex: if baseline SBP ~ 100 + peak SBP after clamp 140, maintain SBP at ~ 120 mmHg • SNP: may MAP distal to AXC + CSFp MHMC Descending Thoracic Aorta Protocol; Anesth Analg 2003;96:SCA1-141
OLV: Left Double Lumen Tube • Provides optimal exposure for descending thoracic aorta surgery: clamp bronchial + ventilate via tracheal lumen • Good margin of safety • Easier to deflate lung (v. blocker) • Bronchial cuff seal volumes + pressures lower (v. blocker) • Easy to apply suction +/or CPAP • Risk of change-over to single lumen ETT • Can withdraw bronchial lumen to mid-tracheal position • Clamp tracheal lumen + ventilate via bronchial lumen Slinger PD: J Cardiothorac Vasc Anesth 1993;7:108-12
Univent • Movable blocker shaft in external lumen of tube • Easier to insert than DLT (e.g., diff airway, C-spine) • Need higher cuff volumes + pressure to seal blocker • Need suction to deflate blocked lung
Pitfalls in Thoracic Aorta Trauma • Failure to appreciate severity of associated injuries • Failure to treat anemia + hyperglycemia • Failure to insure adequate personnel, equipment, blood products • Failure to provide adequate ventilation + adequate oxygen delivery • Failure to provide optimal hemodynamics during + after aortic cross clamp / CPB