Download
1 / 41
450 likes | 1.42k Vues
Fetal Circulation & Fetal Surgery. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Fetal Cardiac Surgery. Seoul National University Hospital. Fetal Cardiac Surgery. Operative Technique (I). Operative Technique (II). Operative Technique (III).

E N D
Fetal Circulation & Fetal Surgery Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Fetal Cardiac Surgery Seoul National University Hospital
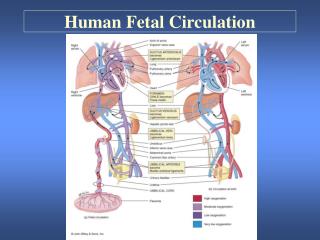
Normal FetalCirculation Percent flow Saturation
Management of the Fetus With a Correctable Congenital Defect
Regulation of Fetal Circulation 1. Local regulation 2. Baroreflex regulation 3. Chemoreflex regulation 4. Autonomic nervous system 5. Hormonal regulation . Catecholamines . Renin-Angiotensin system . Vasopressin . Arachidonic acid metabolites
Isolation of the Placenta during Bypass 1. Placenta remained in bypass circuit ⊙ Advantage . Eliminating an extracorporeal oxygenator . Placenta acts as the gas exchange unit ⊙ Disadvantage . Continuous stimulation of the production of vasoactive substances . Large flow rate 2. Removal of placenta in bypass circuit ⊙ Advantage . Decreased stimulation of vasoactive substances . Reduced required flow rate ⊙ Disadvantage . Oxygenator needed . Effects of arresting placental flow
Fetal Stress Response The ideal fetal anesthesia should be easy to administer, totally block the stress response, not cause fetal myocardial depression, and not disrupt the balance of resistances in various peripheral vascular beds. ⊙ Opiates ⊙ Ketamine ⊙ Halothane ⊙ Total spinal anesthesia (Tetracaine) ** Elevation of various stress hormone, including endogenous catecholamine, release of prostaglandins during fetal surgical exposure and bypass.
Placental Response to Fetal Cardiopulmonary Bypass Placental dysfunction was found to be result of elevated placental vascular resistance ⊙ Pulsatile flow ⊙ Nitroprusside ⊙ Indomethacin : block the arachidonic acid cascade at the cyclooxygenase step ⊙ Corticosteroid : block at the arachidonic acid cascade at the phospholipase step ** Vasoactive cyclooxygenase product (PGE2, Thromboxane) Acute death following fetal bypass is caused by reduced placental blood flow, hypercarbia, hypoxia, lactic acidosis and terminal ventricular fibrillation.
Transvaginal Fetal Echocardiography ⊙ Standard cardiac projection at gestational week 12, and many were imaged by week 11. ⊙ The four-chamber view in 90% of fetuses at 12 weeks?gestation and 100% at 13 weeks. ⊙ Aortic, pulmonary, ductus arteriosus and aortic arch at 12 weeks. ⊙ Mitral & tricuspid valves were resolved in 60% of fetuses by 11 weeks?gestation.
Fetal Intervention forCongenital Heart Disease 1. The ability to diagnose specific lesions in utero 2. A clear advantage to correcting the lesion before birth 3. A technical skills and knowledge to correct safely
Open Fetal SurgicalCorrection in Humans 1. Diaphragmatic hernia 2. Obstructive hydronephrosis 3. Sacrococcygeal teratomas 4. Congenital cystic adenomatoid malformation
Fetal Cardiovascular System 1. The fetus has three vascular shunts. Venous duct Arterial duct Oval foramen 2. The presence in the fetal circulation of the placenta. 3. The lungs in the fetus have high vascular resistance, low blood flow, and provide no gas exchange.
The Placenta The placenta is extremely complex, functioning as the organ of gas exchange, and the primary organ of metabolic and fluid homeostasis, thereby serving the primary roles of the postnatal lung and kidney. The placenta also has important endocrine functions and presents nutrients to the fetal blood stream.
Characteristics of Fetal Circulation 1. There is mixing of the oxygenated and deoxygenated blood. 2. The heart works as a high volume single pumping chamber. 3. The organ of gas exchange is a high volume resistance unit. 4. The myocardium has poor systolic and diastolic function. 5. The fetal cardiac output is very dependant on heart rate. 6. The autonomic nervous and adrenergic system are immature. 7. Myocardial utilization of energy differs in the fetus .
Fetal Blood Flow Patterns 1. Venous return to the heart ⊙ Umbilical-placental blood flow 45% of total fetal cardiac output (200ml/Kg/min) 2. Cardiac output and its distribution. ⊙ Fetal cardiac output 450ml/Kg/min Right ventricle 2/3 Left ventricle 1/3 3. Intracardiac and vascular pressures ⊙ Main pulmonary artery : 55/35 mmHg ⊙ Right atrial pressure : 3~4 mmHg ⊙ Left atrial pressure : 2~3 mmHg ⊙ Umbilical vein pressure : 6~8 mmHg
Advantages ofFetal Cardiac Intervention 1. This restores normal cardiac flow patterns, which result in less secondory maldevelopment 2. A period of time after intervention is provided during which the fetal heart can recover without stress and prepare for the change to postnatal circulation
Advances in Fetal Interventions 1. Refinement of in utero transfusion technique 2. Initiation of pharmacological treatment 3. Introduction of percutaneous catheters 4. Direct fetal exposure and surgical repair
Fetal Intervention 1. Drugs or percutaneous catheter 2. Open fetal surgery ** Common complication . Induction of Labor . Preterm delivery . Mirror syndrome
Maternal Risks of Open Fetal Surgery 1. The operative risks of general anesthesia and a midgestation hysterotomy 2. The risk of premature labor following hysterotomy 3. The risk of compromising future reproductive potentials
Experimental Works forFetal Cardiac Surgery 1. Placental response to fetal cardiopulmonary bypass 2. Fetal stress response 3. Isolation of the placenta during bypass
Nature of Fetal Myocardium ⊙ The cell diameter is smaller, and the ratio of noncontractile mass to the number of contractile myofibrils is significantly greater. ⊙ In fetal myocardium, about 30% of muscle mass is composed of contractile element. ⊙ Isolated fetal myocardium has a lower threshold to the inotropic effects of norepinephrine and is more sensitive to it. ⊙ Fetal myocardium generates less active systolic tension and the resting tension is higher.
Malformations that May Require Intervention in Utero 1. Deficiency states that may be alleviated ⊙ Deficient pulmonary surfactant ⊙ Anemia-erythroblastosis and hydrops ⊙ Hypothyroidism and goiter ⊙ Methylmalonic acidemia ⊙ Multiple carboxylase deficiency ⊙ Nutritional deficiency & intrauterine growth retardation 2. Anatomic lesions that interfere with development ⊙ Hydronephrosis ⊙ Obstructive hydrocephalus ⊙ Diaphragmatic hernia ⊙ Sacrococcygeal teratoma ⊙ Congenital cystic adenoid malformation ⊙ Hydrothorax ⊙ Congenital heart defects
Advantages of In UteroSurgical Therapies 1. Early intervention before irreversible damage is the paramount benifit. 2. The fetal immune surveillance system is not yet intact. 3. Limb buds retain regenerative potential during embryogenesis. 4. Rapid healing, fostered by fetal growth foctor, is characteristic. 5. The umbilicus services both respiratory and nutritional needs without extracorporeal support. 6. Infections are combated by passage of maternal immune factors. 7. Surgical manipulations and postoperative period are simplified. 8. Medicinal agents administered directly to the fetus have greater efficacy at reduced doses.
Potential Advantages of Fetal Surgery 1. The birth of an apparently normal child. 2. The absence of scar. 3. The salvage of compromized vital anatomical structure. 4. The cost effectiveness of a postoperative period in utero.
Pain Perception in Fetus and Neonate 1. Neurochemical system associated with pain ⊙ Tachykinin system ⊙ Endogenous opioid system . enkephalinergic . endorphinergic 2. Physiologic changes associated with pain ⊙ Cardiorespiratory changes ⊙ Hormonal and metabolic change
Background • Intrauterine surgery has become a reality. • Fetal surgical approach might be advantageous to minimize post-natal anatomic deviations for some congenital cardiac lesions. • Better understanding of unique response of the fetus to surgical exposure and extracorporeal circulatory support is mandatory for the successful surgery on the fetus.