Download
1 / 21
240 likes | 364 Vues
Bone Marrow Transplant in Oncology. Dr S D Moodley Wits Donald Gordon Medical Centre. Source. Pathology. Treat Leukemia by chemotherapy Regeneration of normal marrow Chemotherapy alone cannot eliminate all malignant cells Stem cell transplants. Tranplant.

E N D
Bone Marrow Transplant in Oncology Dr S D Moodley Wits Donald Gordon Medical Centre
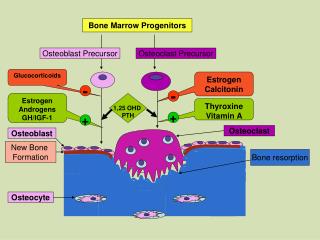
Pathology • Treat Leukemia by chemotherapy • Regeneration of normal marrow • Chemotherapy alone cannot eliminate all malignant cells • Stem cell transplants.
Tranplant • Patient's bone marrow stem cells are replaced with healthy cells • Existing bone marrow and abnormal leukocytes killed • Chemotherapy and radiation • Next bone marrow containing healthy stem cells re-infused
Procedure • Bone Marrow versus Peripheral Stem Cells • Accessibility • Cost • Sample size • Donor/Patient factors • Expertise
Procedure • Most blood stem cells reside in the bone marrow and a small number are present in the bloodstream • Multipotent peripheral blood stem cells • Can be obtained from drawn blood • PBSCs are easier to collect than bone marrow stem cells
Umbilical Cord Blood Stem Cell Transplant • Umbilical cords have traditionally been discarded as a by-product of the birth process. • Pluripotent-stem-cell-rich blood found in the umbilical cord rich in marrow stem cells and PBSC’s.
Umbilical Cord Tx • Umbilical cord transplants are less prone to rejection. • Cells have not yet developed the features that can be recognized and attacked by the recipient's immune system. • Umbilical cord blood lacks well-developed immune cells, there is smaller incidence of graft versus host disease.
THE FUNCTION OF BMT UNIT Handling services & Intensive care for: • Mobilization / stem cell collection & infusion. • Chemotherapy for pre - transplant • Pre & post care for Transplant patients.
Transplantation • Autologous • Allogeneic • Syngeneic
Indications • Hematological diseases Benign : Thallassaemia, Aplastic Anaemia Malignant : Leukemia Lymphoma Myeloma • Immune deficiency disorders Pediatric and Adult • Neurological Disease (MS)
Recovering from the transplant • Recovery of normal levels cells is called engraftment • Day 8 - 12 • Neutrophil engraftment important (GCSF) may be given to accelerate the process • Platelets are the next to return with red cells last. • Commonly patients require transfusion of red cells and platelets following a transplant. • Discharge upon neutrophil & platelet engraftment
Graft Verses Host Disease (GVHD) • GVHD sometimes occurs with allogeneic transplantation. • Lymphocytes from the donor graft attack the cells of the host • GVHD can usually be treated with steroids or other immunosuppressive agents. • Acute GVHD occurs before day 100 post-transplant • Chronic GVHD occurs beyond day 100 • Recent advances have reduced the incidence and severity of this post-transplant complication, but GVHD, directly or indirectly, still accounts for approximately 15% of deaths in stem cell transplant patients • Chronic GVHD can develop months or even years post-transplant
GVHD • Skin/Hair Rash, scleroderma, lichenoid skin changes, dyspigmentation,alopecia • Eyes Dryness, abnormal Schirmer's Test, cornealerosions, conjunctivitis • Mouth Atrophic changes, lichenoid changes, mucositis,ulcers, xerostomia, dental caries • Lungs Bronchiolitis obliterans • GI tract Esophageal involvement, chronic nausea/vomiting, chronic diarrhea, malabsorption, fibrosis, abdomina l pain/cramps • Liver Abnormal LFTs, biopsy abnormalities • Genitourinary Vaginitis, strictures, stenosis, cystitis • Musculoskeletal Arthritis, contractures, myositis, myasthenia, fascities • Hematologic Thrombocytopenia, eosinophilia, autoantibodies
Transplantation • Unit is important • Expertise • Facility Isolation Phoresis Platelet and blood support Motivated patient
Problems • Intensive process that consumes resources • HIV • Donor registry limited • Other health care priorities