Download
1 / 27
270 likes | 278 Vues
The differential diagnosis of chest pain. Features of myocardial infarction. The tactics of the SPM. The principles of prevention and treatment. Associate Professor N.M. Nurillaeva. Signs and symptoms Ischaemic heart disease may be present with any of the following problems :

E N D
The differential diagnosis of chest pain. Features of myocardial infarction. The tactics of the SPM. The principles of prevention and treatment. Associate Professor N.M. Nurillaeva
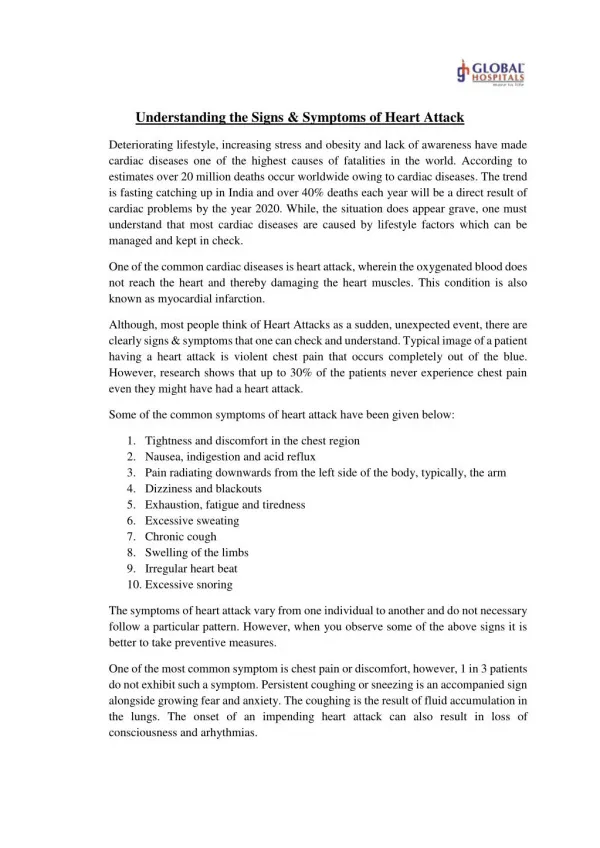
Signsandsymptoms • Ischaemicheartdiseasemaybepresentwithanyofthefollowingproblems: • Anginapectoris (chestpainonexertion, incoldweatheroremotionalsituations) • Acutechestpain: acutecoronarysyndrome, unstableanginaormyocardialinfarction[3] ("heartattack", severechestpainunrelievedbyrestassociatedwithevidenceofacuteheartdamage) • Heartfailure (difficultyinbreathingorswellingoftheextremitiesduetoweaknessoftheheartmuscle)
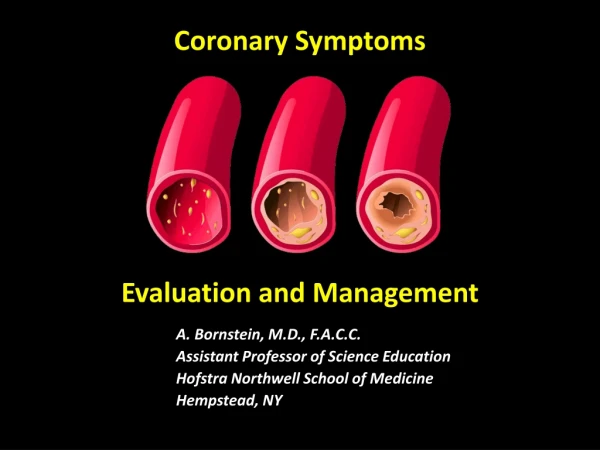
Pathogenesis • Mainarticle: Coronaryarterydisease • Thediseaseprocessunderlyingmostischaemicheartdiseaseisatherosclerosisofthecoronaryarteries. Thearteriesbecome "furredup" byfat-richdepositsinthevesselwall (plaques). • Stableanginaisduetoinabilitytosupplythemyocardium (heartmuscle) withsufficientbloodinsituationsofincreasedcardiacoutput (suchasexertion), andthispainofstableanginanormallyresolveswithrestornitroglicerin (sublingualsprayortablet).
Unstable angina, STEMI and NSTEMI are attributed to "plaque rupture", where one of the plaques gets weakened, develops a tear, and forms an adherent blood clot that either obstructs blood flow or floats further down the blood vessel, causing obstruction there.
Diagnosis of angina is a clinical diagnosis based on a characteristic complaint of chest discomfort or chest pain brought on by exertion and relieved by rest. Confirmation may be obtained by observing reversible ischemic changes on ECG during an attack or by giving a test dose of sublingual nitroglycerin that characteristically relieves the pain in 1 to 3 minutes. Certain tests may help determine the severity of ischemia and the presence and extent of the coronary artery disease. Diagnostic tests may include electrocardiogram (measures electrical activity of the heart), echocardiogram (measures sound waves), exercise-tolerance test, thallium stress test, blood studies to measure total fat, cholesterol and lipoproteins, X-rays of the chest and coronary angiogram (cardiac catheterization).
Signs and symptoms • Ischaemic heart disease may be present with any of the following problems: • Angina pectoris (chest pain on exertion, in cold weather or emotional situations) • Acute chest pain: acute coronary syndrome, unstable angina or myocardial infarction[3] ("heart attack", severe chest pain unrelieved by rest associated with evidence of acute heart damage) • Heart failure (difficulty in breathing or swelling of the extremities due to weakness of the heart muscle)
Stableangina • Mainarticle: Anginapectoris • In "stable" angina, chestpainwithtypicalfeaturesoccurringatpredictablelevelsofexertion, variousformsofcardiacstresstestsmaybeusedtoinducebothsymptomsanddetectchangesbywayofelectrocardiography (usingan ECG), echocardiography (usingultrasoundoftheheart) orscintigraphy (usinguptakeofradionuclidebytheheartmuscle). Ifpartoftheheartseemstoreceiveaninsufficientbloodsupply, coronaryangiographymaybeusedtoidentifystenosisofthecoronaryarteriesandsuitabilityforangioplastyorbypasssurgery.
Mechanism Of Action: NO- Nitrc oxide GC- guanylyl cyclase c-GMP- Cyclic GMPOrganic Nitrates stimulates the intracellular cyclic-GMP, which, results in vascular smooth muscle relaxation of both arterial and venous vasculature. Increased venous pooling decreases left ventricular pressure (preload) and arterial dilatation decreases arterial resistance (afterload). Therefore, this reduces cardiac oxygen demand by decreasing left ventricular pressure and systemic vascular resistance by dilating arteries. Additionally, coronary artery dilation improves collateral flow to ischemic regions.
Область ишемии Область повреждения Область инфаркта
Diagnosis of angina is a clinical diagnosis based on a characteristic complaint of chest discomfort or chest pain brought on by exertion and relieved by rest. Confirmation may be obtained by observing reversible ischemic changes on ECG during an attack or by giving a test dose of sublingual nitroglycerin that characteristically relieves the pain in 1 to 3 minutes.
Acutechestpain • Mainarticles: Acutecoronarysyndromeandmyocardialinfarction • Diagnosisofacutecoronarysyndromegenerallytakesplaceintheemergencydepartment, whereECGsmaybeperformedsequentiallytoidentify "evolvingchanges" (indicatingongoingdamagetotheheartmuscle). Diagnosisisclear-cutifECGsshowelevationofthe "ST segment", whichinthecontextofseveretypicalchestpainisstronglyindicativeofanacutemyocardialinfarction (MI); thisistermed a STEMI (ST-elevation MI), andistreatedasanemergencywitheitherurgentcoronaryangiographyandpercutaneouscoronaryintervention (angioplastywithorwithoutstentinsertion) orwiththrombolysis ("clotbuster" medication), whicheverisavailable. Intheabsenceof ST-segmentelevation, heartdamageisdetectedbycardiacmarkers (bloodteststhatidentifyheartmuscledamage). Ifthereisevidenceofdamage (infarction), thechestpainisattributedto a "non-ST elevation MI" (NSTEMI).
If there is no evidence of damage, the term "unstable angina" is used. This process usually necessitates admission to hospital, and close observation on a coronary care unit for possible complications (such as cardiac arrhythmias – irregularities in the heart rate).Depending on the risk assessment, stress testing or angiography may be used to identify and treat coronary artery disease in patients who have had an NSTEMI or unstable angina.
Stable angina • Main article: Angina pectoris • In "stable" angina, chest pain with typical features occurring at predictable levels of exertion, various forms of cardiac stress tests may be used to induce both symptoms and detect changes by way of electrocardiography (using an ECG), echocardiography (using ultrasound of the heart) or scintigraphy (using uptake of radionuclide by the heart muscle). If part of the heart seems to receive an insufficient blood supply, coronary angiography may be used to identify stenosis of the coronary arteries and suitability for angioplasty or bypass surgery.
Interventions and Practices Considered • Treatment of depression to improve mental health outcomes • Angiotensin-converting enzyme (ACE) inhibitor therapy • Angiotensin II receptor blocker (ARB) therapy • Anticoagulant Therapy • Antiplatelet therapy • Aspirin Clopidogrel • Antiplatelet therapy post stent placement • Clopidogrel plus aspirin • Delay of elective procedures requiring interruption of therapy • Beta-blocker therapy • Atenolol • Bisoprolol • Carvedilol • Labetalol • Metoprolol • Propranolol • Pindolol
Calcium channel blocker therapy • Lifestyle modification • Diet therapy • Dietary fat modification • Smoking cessation • Exercise • Treating comorbid conditions • Hypertension (target blood pressure) • Lipid management (statin therapy) • Interventions considered but not recommended include (1) unopposed estrogen and estrogen and progestin combination therapy for the prevention of cardiovascular events in postmenopausal women; (2) screening for coronary artery disease by exercise stress testing, computed tomography angiography, and coronary artery calcium scoring in asymptomatic adults; and (3) dietary supplement therapy.
Prevention • Some of the risks for heart disease that you CAN change are: • Do not smoke or use tobacco. • Get plenty of exercise -- at least 30 minutes a day, at least 5 days a week (talk to your doctor first) • Stay at a healthy weight. Try for a body mass index (BMI) of between 18.5 and 24.9. • Get checked and treated for depression. • Women at high risk for heart disease should take omega-3 fatty acid supplements. • If you drink alcohol, limit yourself to no more than one drink a day for women, and no more than two drinks a day for men. Because alcohol in large amounts can be toxic to the heart, you may be asked to limit your alcohol even more, or stop drinking it completely. • Good nutrition is important for your heart health and will control some of your risk factors. See also: Heart disease and diet
Примерные формулировки диагноза: • ИБС: стабильная стенокардия напряжения ФК II. ПИКС (2005 г.)(если имеются отразить нарушения ритма и проводимости). Соп: Ожирение: II степени • ИБС: стабильная стенокардия напряжения ФК III. ГБ III стадии, АГ I степени, риск 4 (очень высокий). Фон: СД 2 тип с повышенной массой тела, средней степени тяжести • ИБС: острый коронарный синдром без подъема сегмента ST (далее с трансформацией в прогрессирующую стенокардию, потом в стабильную стенокардию напряжения ФК III). ГБ III стадии, АГ II степени, риск 4 (очень высокий) • ИБС: острый инфаркт миокарда с зубцом Q(от 7авг. 2007г.), подострая стадия с нарушением ритма ЖЭС III кл. по Лауну. Осл.: Отек легких(от 9 авг. 2007г.) • ИБС: острый инфаркт миокарда без зубца Q. Осл: Синд-ром Дресслера (или ранняя постинфарктная стенокардия и т.д.) (указать число). Соп: Ожирение III степени • ИБС: прогрессирующая стенокардия напряжения (далее трансформация в стабильную стенокардию или ИМ). ГБ III стадии, АГ I степени, риск 4 (очень высокий). Осл: НК IIА стадии (II ФК по NYHA)
Management • In stable IHD, antianginal drugs may be used to reduce the rate of occurrence and severity of angina attacks. Treatments for acute coronary syndrome and established coronary artery disease is discussed above in "diagnosis". Revascularization for acute coronary syndrome has a significant mortality benefit.. Recent evidence suggests that revascularization for stable ischaemic heart disease may also confer a mortality benefit over medical therapy alone.[ • Treatment of coronary artery disease includes addressing "modifiable" risk factors. This includes suppression of cholesterol (usually with statins), even in those with statistically normal cholesterol levels, control of blood pressure, blood sugars (if diabetic), and regular exercise. Smokers are encouraged to stop smoking. Diet plays a major role in the progression of coronary artery disease and by making certain diet choices a person can drastically change their chance of dying from it.[
Epidemiology • IHD is the leading cause of death for both men and women in the US and other industrialized countries. It may affect individuals at any age but is most common in older individuals. Males are affected more often than females however the rates equalize between men and women following menopause.