Download
1 / 27
270 likes | 438 Vues
Public Health Practice I: HIV/AIDS Consequences for Socio- Economic Development. Thomas Novotny The World Bank. Outline of Presentation. The Global HIV/AIDS Pandemic HIV/AIDS in Europe and Central Asia Potential economic impact Policy approaches The Balkans, Moldova & Central Asia

E N D
Public Health Practice I: HIV/AIDSConsequences for Socio- Economic Development Thomas Novotny The World Bank
Outline of Presentation • The Global HIV/AIDS Pandemic • HIV/AIDS in Europe and Central Asia • Potential economic impact • Policy approaches • The Balkans, Moldova & Central Asia • Conclusion
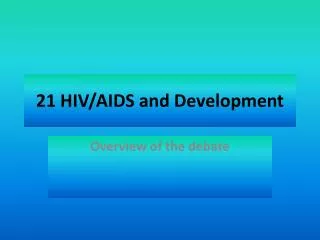
GlobalHIV Pandemic + 1 300% +20% + 20% + 160% + 100% +60% + 40% + 30% + 20% UNAIDS
HIV/AIDS Estimates in ECA (2003) UNAIDS 2003
Epidemic Outlook Eastern Europe and Central Asia confront 4 overlapping epidemics • Drug Use • HIV/AIDS • Sexually Transmitted Infections • Tuberculosis Epidemic drivers act regionally and can best be addressed at regional level • Trafficking in people and drugs • Economic and political migration • Sex Work • Prisons Godinho J, Renton A, Vinogradov V, Novotny T, Gotsadze G, Rivers MJ, Bravo M (2004)
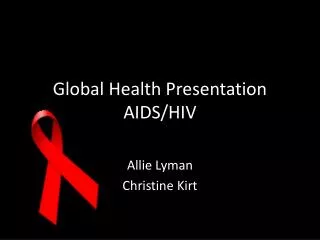
Explosive Epidemics of HIV among IDU 80 Myanamar 60 Samara RF Edinburgh Manipur 40 HIV prevalence (%) Bangkok 20 Odessa 0 2001 1997 1999 1987 1989 1991 1993 1985 1983 1995 Year Renton A 2004
High STI Prevalence Low STI Prevalence 10 explosive IDU epidemic 20 larger sexually transmitted epidemic 10 explosive IDU epidemic Smaller and slower 20 sexually transmitted epidemic No IDU harm reduction Contained IDU epidemic Smaller and slower 20 sexually transmitted epidemic Contained IDU epidemic Very small and slow 20 sexually transmitted epidemic Successful IDU harm reduction STI/IDU/HIV Interactions Renton A 2004
Role of HIV/AIDS in Fueling the TB epidemic • Socio-structural Factors • Over-crowded prisons • Poverty related commercial sex • Sale and transfusion of • contaminated blood • Epidemiological Factors • Prevalence of TB in PLWH • MDR-TB Prevalence in PLWH • Duration of infectiousness in PLWH • STI and other co-morbidities • Lack of access to • HAART • STI Treatment • Harm Reduction for IUD • Condom Use TB TRANSMISSION TB INFECTION ACTIVE TB CURE RECURRENCE DEATH TB Preventive Treatment Access to Second-line drugs Intensified case-finding Decreased delay in case detection and DOTS TB Preventive Treatment BCG Interventions to avert the TB epidemic fueled by HIV/AIDS
HIV/AIDS Role in Poverty Contributors to Poverty • Loss of income • Catastrophic cost of care • Increased dependency ratio • Loss of productivity (companies) • Loss of social capital (countries) • Reduced national income? HIV Infection AIDS
Epidemic Drivers Economic & Political migration Low Level HIV Epidemic Explosion of Injecting Drug Use Poverty/ Income Differentials Unemployment Explosion of Commercial Sex Work Drug Trafficking Concentrated HIV Epidemic Low levels of population awareness and knowledge of HIV & STI Epidemics of STIs Low levels of population awareness and knowledge of HIV & STI Generalized HIV Epidemic Renton 2004
Potential Economic Impact in Russia • Economic growth rates could decline by 0.5-1.0 percent annually • Health expenditures could increase up to 50 percent • Costs of treatment would not be sustainable • The dependency ratio could rise • Household size & composition could change • Transfer of intellectual capital and social skills from one generation to another could be lost Ruhl C, Pokrovsky V, Vinogradov V 2002
Decriminalize risk behavior Improve medical treatment Social support to PLWHA Legislative authority for NGOs to work with vulnerable groups Reproductive health & HIV/AIDS Education IDU, CSW, MSM, Migrants Narcology, HAART, STIs, TB Social protection, palliative care Harm Reduction, outreach Schools,policymakers, general public Policy Approaches
Sentinel surveillance of high risk groups Behavioral Serologic Respondent-driven sampling Venue-based testing Voluntary testing and counseling Data used for decision making Harm reduction Education programs Supply chain for drugs, supplies, condoms Prison health system National AIDS Programs Information Needs Monitoring Evaluation
Non-financial Factors • Political will and perception • Social constraints and stigmatization • Community, Gender, and Values • Institutional capacity to implement effective interventions • Regulatory and legal issues • Donors Coordination
Funding Needs • Funding would have to increase from $300 million in 2001 to $1.5 billion in 2007 • 40% for prevention • 55% for care and treatment • 5% for policy, administration, research & evaluation • For treatment of HIV/AIDS & TB, funding would have to increase • For ARVT, from $60 million in 2002 to more than $600 million by 2007 • For TB control, from <1 billion in 2001 to $1.9 billion by 2007 UNAIDS and The World Bank 2003
HIV/AIDS in ECA Countries • Opportunity for prevention is now • Cross-border externalities important in addressing most vulnerable groups • Future burden on health systems and economic productivity may be enormous • Sentinel surveillance in high risk groups and vulnerable populations is needed • Harm reduction application and decriminalization are needed • Public information and professional education are essential
Youth Vulnerability • 80% of infected persons are less than 30 years of age in ECA • Primary carriers are boys and young men • CSW and trafficking in girls and young women • IDU, heavy alcohol use, and lack of access to reproductive health education and safe sex • Iatrogenic cases in Romania
Mobile Populations • Sailors, truckers (37% have unsafe sex while traveling) • Peacekeepers • Commercial Sex Workers (CSW) • Trafficked women and children • Roma and other ethnic minorities (8 million in ECA) • Displaced people • Tourists
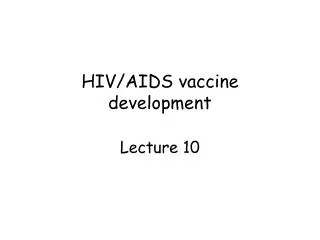
Is Harm Reduction working in Moldova? New Cases Laticevschi D 2004
Drug and migration routes Red: high risk oblasts, major drug routes Green: human trafficking routes Renton A, Gzirishvili D, Gotsadze G, Godinho J 2004
Results Prevention Needs US$208 million Treatment Costs US$??? million per year + Existing Resources: 2002 to 2010 US$75 million Given needs outweigh resources what is best way to spend the money? Cercone 2004 J 2004
AIDS Challenges in ECA • Target most vulnerable groups with appropriate approaches • Improve Public Health functions • Increase opportunities for youth to participate in the knowledge economy