Download
1 / 19
200 likes | 540 Vues
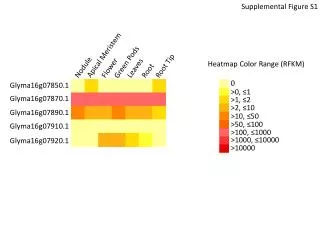
CYST-MURAL NODULE. Differential diagnosis: Pilocytic astrocytoma Pleomorphic xanthoastrocytoma Ganglion cell tumors Hemangioblastoma. FREQUENTLY CALCIFIED TUMORS. Oligodendroglioma Pilocytic astrocytoma Subependymal giant cell astrocytoma Ependymoma/ subependymoma

E N D
CYST-MURAL NODULE Differential diagnosis: • Pilocytic astrocytoma • Pleomorphic xanthoastrocytoma • Ganglion cell tumors • Hemangioblastoma
FREQUENTLY CALCIFIED TUMORS • Oligodendroglioma • Pilocytic astrocytoma • Subependymal giant cell astrocytoma • Ependymoma/ subependymoma • Choroid plexus papilloma • Ganglion cell tumor • Central neurocytoma • Pineal cyst • Meningioma • Craniopharyngioma • Vascular malformations • Retinoblastoma
NEOPLASTIC CYSTIC LESIONS • Pilocytic astrocytoma • Ganglion cell tumors • Desmoplastic infantile ganglioglioma • Ependymoma • Hemangioblastoma • Pleomorphic xanthoastrocytoma • Craniopharyngioma • Meningioma (occasional) • Schwannoma (usually large ones)
INTRAVENTRICULAR TUMORS • Ependymoma (lateral, 3rd, 4th) • Subependymoma (lateral, 4th) • Subependymal giant cell astrocytoma (lateral) • Choroid plexus tumors (lateral, 3rd, 4th) • Pilocytic astrocytoma (lateral, 3rd, 4th) • Central neurocytoma (lateral, 3rd) • Papillary craniopharyngioma (3rd) • Colloid cyst (3rd) • Meningioma (lateral, 3rd, 4th)
REACTION OF NEURON TO INJURY Acute neuronal injury: • Shrinkage of cell body, pyknosis of nucleus, disappearance of the nucleolus, loss of Nissl substance, intense eosinophilia of cytoplasm Red Neuron Subacute & chronic neuronal injury: • Degeneration- cell loss often selective, reactive gliosis Axonal reaction: • Regeneration of the axon- enlargement & rounding up of cell body, peripheral displacement of nucleus, dispersion of nissl substance to the periphery of cell Subcellular alterations: • Neuronal inclusions, neurofibrillary tangles.
REACTION OF ASTROCYTES TO INJURY • Gliosis: hypertrophy & hyperplasia of astrocytes. • Gemistocytic astrocyte: Nucleus of astrocyte enlarges, prominent nucleolus, cytoplasm expands becomes bright pink and irregular displacing nucleus to periphery • Rosenthal fibers: thick elongated brightly eosinophilic structures with irregular contours, within astrocytic processes • Corpora amylacea: polyglucosan bodies faintly basophilic PAS positive concentrically lamellated
BRAIN PARENCHYMAL INJURIES • CONCUSSION • CONTUSIONS-coup and countrecoup • LACERATION
INFLAMMATORY DISEASES • DEMYELINATING DISEASES-multiple sclerosis • IDIOPATHIC INFLAMMATORY & REACTIVE DISORDERS • XANTHOMATOUS LESIONS • HISTIOCYTOSES
MULTIPLE SCLEROSIS Presentation: May present as space occupying tumors with mass effect, edema and disruption of blood brain barrier, neurological deficit due to involvement of cranial nerves, spinal cord lesion cause sensory/motor impairement • CT MRI : diffuse / ring-like enhancement • Gross: Lesions sharply delineated from adjacent white matter. • Microscopy: Diffuse infiltration of foamy macrophages, reactive astrocytosis, perivascular aggregates of small lymphocytes and plasma cells • Pathogenesis: Cellular immune response against components of myelin sheath, demyelination casused by activated macrophages • CSF EXAM- mild elevation of protein , moderate pleocytosis, gamma globulin increased most patient shows oligoclonal bands
INFARCTION • Cerebral blood flow—50 ml/min per 100 gm of tissue. • Two principal types of ischemic injury • GLOBAL CEREBRAL ISCHEMIA • FOCAL CEREBRAL ISCHEMIA
GLOBAL CEREBRAL ISCHEMIA • Cause: (diffuse ischemic encephalopathy) generalized reduction of cerebral perfusion e.g. shock cardiac arrest, severe hypotension • Morphology: Swollen brain, widened gyri, narrowed sulci, little demarcation b/w white and gray matter • Early changes12-24 hrs: acute neuronal cell change- red neurons, microvacuolization, cytoplasmic eosinophilia, nuclear pyknosis and karyorhexis. These changes later appear in astrocytes and glial cells. infiltration of neutrophils • Subacute changes 24hrs-2wks: necrosis, influx of macrophages, reactive gliosis and vascular proliferation. • Border zone (water shed) infarct: wedge shaped , lie at most distal fields of arterial irrigation
FOCAL CEREBRAL ISCHEMIA Cerebral arterial occlusion resulting in ischemia and infarction in a specific region within the territory of distribution of the compromised vessel Causes: • Thrombosis • CADASIL • Cerebral amyloid angiopathy • Embolism 1. THROMBOSIS: majority due to atherosclerosis, • Sites : carotid bifurcation, origin of middle cerebral artery, basilar artery • Predisposing factors: Arteritis due to syphilis and tuberculosis, polyarteritis nodosa and primary angitis of CNS; hypercoagulable states, dissecting aneurysm and drug abuse are other causes.
FOCAL CEREBRAL ISCHEMIA • CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy • Morphology: concentric thickening of adventitia and media of cerebral and leptomeningial arteries. • Basophilic PAS positive granules in walls of vessels also in other sites like skin or muscle biopsies. • CEREBRAL AMYLOID ANGIOPATHY: • deposits of amyloidogenic peptides Aβ40 in walls of small and medium sized vessels • EMBOLISM : • Predisposing factors: cardiac mural thrombi, MI , valvular disease, atrial fibrillation, atherosclerotic thrombi, paradoxical emboli. • Site: Territory of middle cerebral artery is most frequently affected
Focal infarction with punctate hemorrhages caused by an embolus