Download
1 / 24
240 likes | 354 Vues
Logo for TMF Health Quality Institute appears in the upper left hand corner of each slide in this presentation. The Model for Improvement A Method to Adapt, Implement and Spread Change. Melody Malone, PT Quality Improvement Consultant Hello! I am pleased to be joining you.

E N D
Logo for TMF Health Quality Institute appears in the upper left hand corner of each slide in this presentation.The Model for ImprovementA Method to Adapt, Implement and Spread Change Melody Malone, PT Quality Improvement ConsultantHello! I am pleased to be joining you. By being at this presentation today you have chosen to make a difference in the lives your Residents, their families, your staff and in the way you practice your professions. As your quality improvement progresses you will have a unique opportunity to spread what you will learn not only within your facilities but out into the larger community. You are taking the steps necessary to move us from where we are; to where we want and should be. Throughout your quality improvement efforts, never loose site that YOU are the vehicle, the fuel, that makes all this possible. Without you there is no change! Let’s discuss The Model for Improvement - A Method to Adapt, Implement and Spread Change, through something we call P.D.S.A.
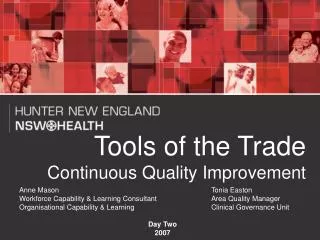
Act Plan Study Do Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? The Plan – Do – Study – Act Cycle is a way for us to systematically go through quality improvement in a thoughtful way. It starts with 3 questions. Once we have asked AND answered the three questions we are ready to go to work. But before we can go to work we need a well thought-through plan. Let’s start by reviewing the 3 questions…
Model for Improvement What are we trying to accomplish?First, What are we trying to accomplish? Have you ever attempted to take a trip without asking “Where are we trying go?” The best way to answer this to set up a goal statement.
Q 1: What are we trying to accomplish? A: Goal Statement A written statement of accomplishments expected from each pilot team’s improvement effort. Contains useful information: • A general description of the goal • A specific population • Numerical goals A general description of spreadThe goal statement is going to layout what the team expects to accomplish in the QI project. It will act as a guide to help keep you on track. An example of a goal statement might be: To improve satisfaction level of the residents we will commit to consistent staff assignments on Unit 1 within 30 days AND we will spread this change throughout each unit within 1 quarter. The team that developed this goal statement is pretty clear as to what the goal is, who they are going to work with, what the measurable goals are and that they hope to spread it beyond just their team.
Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement?The second question we need to answer in order to get ready is How will we know that a change is an improvement? Versus a set back.
Q 2:How will we know that a change is an improvement? A: Measurement • Each PDSA cycle • Each monthly key measure Each spread measureYou have an opportunity at the end of each P.D.S.A. cycle to study what has happened and check it against your goal statement. Each month you have a myriad of data available to you that you can use as key measures, such at the Quality Measures, Quality Indicators and turnover data. You might need to develop a specific key measure that you will use to measure the success of the test of change. Plotting on run charts your key measures will help you visually see the progress, or lack of progress, that this change is making. Use a balanced set of at least 3 measures to assure that the system is improved.
Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement?And the third question is What change can we make that will result in improvement?
Q 3:What changes can we make that will result in an improvement? A: Improvement Strategies Identified through: • A change package • Resident input/ideas • Satisfaction surveys • Chart audits BrainstormingThis can be done through developing strategies aimed at reaching an improvement. A strategy may be just a simple idea someone has for making things better. It doesn’t have to be some big “rocket science” thing. Don’t forget there is also a larger community to pull from for ideas. The Long Term Care Community has other resources, standards of care, providers and many other resources. Embrace them in your efforts. As outcomes improve, you move closer to an optimal quality of life of both the Residents and your staff. The two work very closely together.
Act Plan Study Do Model for Improvement What are we trying to accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement?Now I am going to discuss the Plan – Do – Study – Act Cycle. Once we have asked the three questions we are ready to go to work. First we need a thoughtful plan that will helps us take the three questions and put them to work. That work is: Testing or adapting a change Implementing an improvement on a small scale, then Spreading the improvements to the rest of your organization
The PDSA Cycle for Learning and Improvement Act What changes are to be made? Next cycle? Plan Objective Questions and predictions (why) Plan to carry out the cycle (who, what, where, when) Do Carry out the plan Document problems and unexpected observations Begin analysis of the dataContrast this model with P-P-P-Panic: Plan, Plan, Plan, Panic! You can never plan for all things that MIGHT happen. But don’t let that keep you from taking action! Plan: Each PDSA cycle has an objective and a measure. Learn from predictions. DO: Do the plan & collect data but WE HAVE TO COLLECT THE RIGHT DATA Study: test hypothesis. Power of learning is in the things we didn't expect. P-D-S is scientific method. Act: what are we going to do next? Plan-Do is a common problem. If don't study, never know if it works. Some teams Do-Do-Do-Do: good news, get a lot done. Bad news: sometimes find yourself in failures These things are not PDSA cycles: (unless they test different ways) : Meetings specific tasks: revise a form improving a global measure a plan to accomplish each goal Reasons for failed tests 1. Change not executed well 2. Support processes inadequate 3. Hypothesis/hunch wrong: - Change executed but did not result in local improvement - Local improvement did not impact global measure Collect data during the ‘Do’ phase of the cycle to help differentiate these situations. Do-Study can be tough. Example #1 tests that didn't work: Restraint reduced but staff didn’t follow-thru with plan Example #2: weekly skin checks but have residents who refuse Example #3: implementing consistent staffing, but failed to include housekeepers. Can't say it didn't work and stop there. Need to understand why. Doesn't mean concept was wrong. Conclusions are important. Document why it failed, build PDSA skills Celebrate failures--gold mine in your QI efforts. Share with others on your team, in the facility and in the LTC world. Study • Complete the analysis of the data • Compare data to predictions • Summarize what was learned
Purpose: Increase protein in residents’ diet Plan: Add protein powder to all dessert recipes To Do: Collect data Educate staff Experiment with recipes Purchase protein powderHere is an example of a Small-Scale, Rapid PDSA Cycle And note, you can include the residents by letting them help to sample the desserts. Try it even if you think the solution might fail – TRY IT AND LEARN FROM IT! Small-Scale, Rapid PDSA Cycle
Small-Scale, Rapid PDSA cycle continued Do: Study: Act: • Adopt? • Adapt? • Abandon?Once you get to the ACT stage you have to decide are going to: 1. Adopt? 2. Adapt? Or 3. Abandon? This idea? If you AdOptit then you move to a next Small-Scale, Rapid PDSA cycle to roll it out to in a larger scale – maybe a new group of staff or residents. The whole unit? If you AdAptit then you move to a next Small-Scale, Rapid PDSA cycle to test the change in the plan If you Abandon the idea WHAT DID YOU LEARN FROM IT?
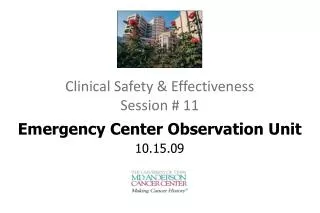
A P S D D S P A A P S D A P S D Repeated Use of the Cycle DATA Spread Implementation of Change Wide Scale Tests of Change Follow-up Tests Very Small Scale Test Changes That Result in ImprovementI have an idea, I'd like to make it work. Start with a small test (example: fall risk program on the next new admission) Do a follow-up test. To rework as you learn & get more specific. Do a wider-scale test, tougher more patients, more risk (different culture, different providers) implement at the top. Spread on a wider scale - to hospitals, Ambulance company, other Nursing homes in your company, or in your community. Not one test, many tests Like learning an instrument. You keep learning and gaining confidence because of a lot of learning. Deal with special circumstances, such as weekends, days on which you have a lot of admits.! Many of you will do multiple tests before you come up with a system you feel is fool proof. Hunches Theories Ideas Spread Implementation of Change Wide Scale Tests of Change Follow-up Tests Very Small Scale Test
Cycles for Testing ChangesPurpose: Cycle 1 - Cycle 2 - Cycle 3 - Cycle 4 - Cycle 4 - Cycle 5 –Model component: Fall Risk Maybe you start with you frequent faller. Learn and gain confidence from him then move to all fallers on his unit, then all fallers in the facility, then to all new admits, then to the pre-admission hospital setting to give them some ideas of how to handle the residents without restraints!
Why Test? To answer questions… • Will change result in improvement? • How much improvement? • Need to adapt the change? • Any costs and/or side-effects? Other reasons… • Opportunity for “failures” Minimizes resistance upon implementationThe ideas are great, but "how" is on trial. Will the change result in improvement? Such as: for PU prevention decide to put cushions in all wheelchairs, this caused an increase in falls – why? Chairs no longer fit the resident. Learned rehab needed to be involved for: proper fit, better cushion selection, perhaps a different program such as w/c pushups or a walking program and they bought too many cushions that they couldn’t use and not enough of the ones they needed. How much improvement? – it may work for some, and on others not at all, such as Alzheimer's residents. More learning Share failures with others "I'm convinced this works, but don't know how much." Will this work in my organization? Build a business case Best use is the last bullet. People love to run tests and give feedback. Won't want to go back to the old way. "Will you test this on 2 residents?“ Share openly and steal shamelessly Failures – in a restraint reduction the resident fell, the staff thought the trial failed. But under examination (study) we discovered multiple communication failures so that the plan for monitoring and intervention did not work. We failed the resident, NOT THAT THE RESIDENT FAILED THE REDUCTION. YOU NEVER WANT TO HAVE A FAILURE ON A LARGE SCALE!
Why not start with implementation? • The change is permanent - need to develop all support processes to maintain change. • High expectation to see improvement (no failures). • Increased scope will lead to increased resistance. • Generally takes more time than tests.There is a difference between testing and implementing. Testing let you work the bugs out Implementing requires finalizing policy, procedures, Example: rewrite job descriptions Tests were with volunteers. Some people may never implement, but they will test. Not days (AS IN TESTING),IMPLEMENTATION IS now weeks to months. This will help with continued compliance vs in and out of compliance “getting ready for survey” Because as we test, we learn and we gain a commitment of others to the new process.
Successful Cycles to Test and Adapt Changes • Scale down size of test (# of residents, location) • Conduct multiple cycles to test & adapt change • Test with volunteers • Do not try to get buy-in, consensus, etc. • Be innovative to make test feasible • Collect useful data during each test • Test over a wide range of conditionsHow quickly you run first cycle determines how successful you will be. Need to successfully plan ahead. No "just-in-case" data. We can always do our little test again. Implementing a plan in your setting may take multiple PDSA cycles, what can you do tomorrow to start testing how to do it. Try on a busy day, in a different season, different setting.
Decrease the Time Frame for a PDSA Test Cycle • Years • Quarters • Months • Weeks • Days • Hours • Minutes Drop next down two levels to plan test cycle!Start with year, turns into a month. If you started thinking you could do it in a quarter, you would need to be thinking next week. If you heard from your team we can to that in a month, what should you say? What could we do in the next day? It's possible to try things quickly and with a few people.
P P P P P A A A A A D D D D D S S S S S S S S S S D D D D D A A A A A P P P P P A A A A A P P P P P S S S S S D D D D D P P P P P A A A A A D D D D D S S S S S Community Involvement Care Practices Assessment of Depression PU Prevention Strategies Staff Turnover Overall Goal: Implement the Model for Improvement at Your Nursing HomeCommunity InvolvementCare PracticesAssessment of DepressionPU Prevention StrategiesStaff Turnover Develop Strategies for Each Component of the ModelYour assignment: Think about all the ideas from in the 5 areas – maybe you have other key issues that you can substitute for the areas. You need to be working on multiple areas of improvement at 1 time - Can't do sequentially, there's not enough time. Keep this in front of you while working. This is not simple--do
GOAL – Improve outcomes Concept AConcept B Concept D Concept C Change Concepts, Theories, IdeasFor some people this is a better mental model Concept D Concept C Concept B
Act Plan Study Do Improvement by NEXT Week! Willing to compromise on • scope, • size, • strictness, and sophistication, but the cycle should include one resident or staff member and must be completed within a week of answering the 3 questions.I want all of you to be successful. If there is one thing I could get you to do, it would be to do your first PDSA cycle. Using the methodology of small scale, rapid cycle PDSAs, conduct your first PDSA as it applies to your system. Use the worksheet as a guide. Remember your goal is: Testing or adapting a change Implementing an improvement Spreading the improvements to the rest of your organization
The Power of One…In statistics we usually look for a sample population of no less than 30, but in long term care we rarely have the opportunity to define a pilot population of 30-100 cases unless we are looking at the full facility census. This is the beauty of using run charts and data for quality improvement! If you have a small number say less than 20 then consider defining your pilot as 100% of the cases. Chances are that if your volume is low, then you have fewer staff or less variation in the types of interventions offered. And the best news is that even one resident can provide information for quality improvement. Let me tell you a story I heard about from the IHI National Forum meeting in December of 2002. A mother is interrupted when her 8 year old daughter comes in crying. The child has two skinned knees, a tear in her shirt, dirt on her face and abrasions on both hands. The mother rushes over to examine the damage asking “what happened to you?” Well, says the little girl, I learned that I shouldn’t ride my bicycle down big hills. I got going too fast and flipped my bike. Immediately, the mother who had background in statistics and used to challenging her QI department on their data replies – “Now, honey, everyone knows that you can’t have a sample size of one. We are going to have to put you back on that bike and send you down the hill at least 29 more times in order to get even close to a decent sample size. Better yet, we are going to have to get some of your friends, of equal riding capabilities of course, to ride down that same hill. And we will record the number of times that you and your friends crash, adjusting of course for abrasions. Can you imagine if the first time you had a bike accident, that’s what your mother said to you? There is power in a sample of one – remember we aren’t doing statistics here, we are using measurement for quality improvement. Now, don’t get me wrong, I certainly appreciate the need for statistics, but not necessarily in this effort.We are striving for quality improvement; we need to learn from each and every opportunity for improvement!image of bicyclist
The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. G. Langley, K. Nolan, T. Nolan, C. Norman, L. Provost. Jossey-Bass Publishers., San Francisco, 1996, Chapter 6. • Quality Improvement Through Planned Experimentation. 2nd edition R. Moen, T. Nolan, L. Provost, McGraw-Hill, NY, 1998. • “Accelerating the Pace of Improvement - An Interview with Thomas Nolan,” Journal of Quality Improvement, Volume 23, No. 4, The Joint Commission, April, 1997. • “Understanding Variation”, Quality Progress, Vol. 13, No. 5, T. W. Nolan and L. P. Provost, May, 1990.
Prepared with assistance from Qualis Health, Lloyd Provost, Associates in Process Improvement and the Institute for Healthcare Improvement. This material was prepared by TMF Health Quality Institute, the Medicare Quality Improvement Organization for Texas, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 8SOW-TX-NHQI-06-10