Download
1 / 34
360 likes | 577 Vues
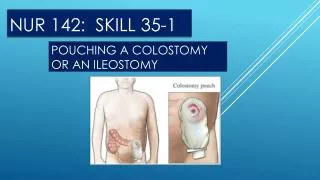
NUR 111 SKILL 7-1 HAND HYGIENE. Hand hygiene - introduction. Infection prevention and control practices that reduce or eliminate sources and transmission of infection help to protect patients and health care providers from disease.

E N D
Hand hygiene - introduction • Infection prevention and control practices that reduce or eliminate sources and transmission of infection help to protect patients and health care providers from disease. • Patients in all health care settings are at risk of becoming colonized or infected as a result of an impaired immune response, exposure to an increased number of pathogenic organisms, and performance of invasive procedures. • Health care-associate infections (HAIs) result from delivery of health service in a health care setting and were not present at the time of admission.
Hand hygiene– cont’d • A hospital is one of the most likely settings for acquiring an HAI because staff, patients, and environmental factors support a high population of pathogens that are resistant to antibiotics. • Health care workers transmit many HAIs by direct contact during the delivery of care. Although protecting patients from HAIs is an obvious priority, nurses are also at risk because of contact with infectious materials or exposure to a communicable disease. • The presence of a pathogen does not mean that an infection will occur.
HAND HYGIENE – cONT’D • Infection occurs in a cycle, often referred to as the chain of infection, which depends on the presence of all of the following elements: • 1. An infectious or pathogen • 2. A reservoir or source for pathogen growth • 3. A portal of exit from the reservoir • 4. A mode of transmission • 5. A portal of entry to the host • 6. A susceptible host An infection develops if this chain remains intact. In patient care it is important to use infection control practices to break an element of the chain so as not to transmit infection.
Hand hygiene – introduction – cont’d • Steps taken to minimize the onset and spread of infection are based on asepsis and the principles of aseptic technique. • Asepsis is the absence of pathogenic (disease-producing) microorganisms. • The two types of aseptic techniques that nurses practice are medical and surgical asepsis. • Medical asepsis, or clean technique, include procedures used for reducing the number of organisms and preventing their transfer.. • Hand hygiene, barrier techniques, and routine environmental cleaning are examples of medical asepsis.
HAND HYGIENE – CONT’D • Principles of medical asepsis are common in the home, as in the case of washing hands before preparing food. • Surgical asepsis, or sterile technique, includes procedures used to eliminate all microorganisms from an area. • Sterilization destroys all microorganism and their spores. • Nurses in the operating room, labor and delivery area, and procedural areas practice sterile technique when using sterile instruments and supplies. • Use sterile technique on nursing units when performing certain invasive procedures (e.g., insertion of a central line or an indwelling urinary catheter). • The techniques for maintaining surgical asepsis is more rigid than those performed under medical asepsis.
EVIDENCED BASED PRACTICE • For generations hand-washing with soap and water was considered the best method to prevent transmission of infection from health care workers to patients. • However, recent research shows that hand-washing with plain soap sometimes results in paradoxical increases in bacterial counts on the skin. • Alcohol-based products are more effective for standard hand-washing or hand antisepsis than soap or antiseptic soaps. • Alcohol-based hand sanitizers reduced infections in a variety of settings from intensive care units to long-term care facilities.
Evidenced-based practice – cont’d • Moreover, brisk alcohol-based rinses or gels containing emollients cause substantially less skin irritation and dryness than plain or antimicrobial soaps. • Soap and water are still necessary for hand hygiene if hands are visibly soiled or when caring for patients infected with Clostridium difficile or multidrug-resistant organisms such as methicillin-resistant Staphylococcus aureus or vancomycin-resistant enterococcus.
EVIDENCED-BASED PRACTICE – CONT’D • Studies show that health care workers with chipped nail polish or long or artificial nails have high numbers of bacteria on their fingertips. • Health care workers should not wear artificial nails and extenders. • No rings or bracelets should be worn during patient care. • Fingernails should not be longer than 0.625 cm (1/4 inch) in length and nail polish should not be chipped. There are no recommendations regarding nail polish color. • Whenever possible, use alcohol-based products that contain emollients.
Patient centered care • As a nurse you are responsible for educating patients about infection prevention. • Patient and family teaching needs to include information concerning signs and symptoms of infection, modes of transmission, and methods of prevention. • Knowledge of the infectious process, disease transmission, and critical thinking skills associated with use of aseptic techniques and barrier protection is essential. • When a patient requires isolation in a private room, remember that loneliness can easily develop.
PATIENT CENTERED CARE – CONT’D • Isolation disrupts normal social relationships with visitors and caregivers. • Some patients who suffer from an infectious disease also experience self-concept or body image changes. • Other cultures rely on alternative health care practices (e.g., the use of Chinese herbs to treat illness and optimize health).
PATIENT CENTERED CARE – CONT’D • When a patient from another culture requires isolation, use caution to be sure that the patient and family understand the therapeutic purpose of isolation. • For example, the isolation of a loved one is considered disrespectful and uncaring behavior in collectivistic cultures (Hispanics, Africans, and Asians). • Unless you act to minimize feelings of psychological and physical isolation, the patient’s emotional state could interfere with recovery.
Safety guidelines • 1. Hand hygiene with an appropriate alcohol-based hand antiseptic or soap and water is an essential part of patient care and infection prevention. • 2. Always know a patient’s susceptibility to infection. Age, nutritional status, stress, disease processes, and form of medical therapy can place patients at risk. • 3. Recognize the elements of the chain of infection and initiate measures to prevent its onset and spread. • 4. Consistently incorporate the basic principles of asepsis into patient care. • 5. Ensure that patients cover their mouth and nose when coughing or sneezing, use tissues to contain respiratory secretions, and dispose of tissues in the waste receptacle.
SAFETY GUIDELINES – CONT’D • 6. Use clean gloves when you anticipate contact with body fluids, non-intact skin, or mucous membranes when there is a risk of drainage. • 7. Use gown, mask, and eye protection when there is a splash risk. • 8. Protect fellow health care workers from exposure to infectious agents through proper use and disposal of equipment. • 9. Be aware of body sites where HAIs are most likely to develop (e.g., urinary or respiratory tract). This enables you to direct preventive measures.
Beginning of skill • The most important and basic technique in preventing and controlling transmission of infection is hand hygiene. • Hand hygiene is a general term that applies to hand-washing, antiseptic hand wash, antiseptic hand rub, or surgical hand antisepsis. • Hand-washing refers to washing hands with plain soap and water. • An antiseptic hand wash is defined as washing hands with water and soap or other detergents containing an antiseptic agent. • An antiseptic hand rub means applying an antiseptic hand rub product to all surfaces of the hands to reduce the number of microorganisms presents. • Surgical hand antisepsis is the use of an antiseptic hand wash or antiseptic hand rub before surgery by surgical personnel to eliminate transient and reduce resident hand flora.
Beginning of skill – cont’d • Antiseptic detergent preparations often have persistent antimicrobial activity. • The decision to perform hand hygiene depends on four factors: • 1. The intensity or degree of contact with patients or contaminated objects. • 2. The amount of contamination that may occur with the contact. • 3. The patient or health care worker’s susceptibility to infection. • 4. The procedure or activity to be performed.
Beginning of skill – cont’d • Longtin et al. (2011) found that hand-hygiene compliance among health care workers found an overall compliance rate below 40%. • Hand hygiene is not optional. It is a critical responsibility for all health care workers. • Follow these guidelines for hand hygiene (CDC, 2001; WHO 2009): • 1. Wash hands with either plain soap and water or an antibacterial soap and water when hands are visibly dirty, soiled with blood or other body fluids, before eating, and after using the toilet. • 2. Wash hands if exposed to spore-forming organisms such as Clostridium difficile or Bacillus anthracis.
BEGINNING OF SKILL – CONT’D • 3. If hands are not visibly soiled, use an alcohol-based hand rub for routinely decontaminating hand in the following clinical situations: • A. Before and after having direct contact with patients. • B. Before applying sterile gloves and inserting an invasive device such as an indwelling urinary catheters and peripheral vascular catheters. • C. After contact with body fluids or excretions, mucous membranes, and non-intact skin. • D. After contact with wound dressings (if hands are not visibly soiled). • E. When moving from a contaminated body site to a clean body site during patient care. • F. After contact with inanimate objects (e.g., medical equipment) in the immediate vicinity of a patient. • G. After removing gloves.
assessment • 1. Inspect surface of hands for breaks or cuts in skin or cuticles. Cover any skin lesions with a dressing before providing care. If lesions are too large to cover, you may be restricted from direct patient care. • Open cuts or wounds can harbor high concentrations of microorganisms. • Agency policy may prevent nurses from caring for high-risk patients if open lesions are present on hands (WHO, 2009). • 2. Inspect hands for visible soiling. • 3. Inspect condition of nails. Natural tips should be no longer than 0.625 cm (1/4 inch) long. Be sure that fingernails are short, filed, and smooth. • Subungual areas of hands harbor high concentrations of bacteria. • Long nails and chipped or old polish increase the number of bacteria residing on hands. • Artificial applications increase microbial load on hands (Boyce and Pittet, 2008, CDC, 2002).
planning • 1. Expected outcomes following completion of procedure: • Hands and areas under fingernails are clean and free of debris • Transient bacteria have been removed
implementation • 1. Push wristwatch and long uniform sleeves above wrists. Avoid wearing rings. If worn, remove during hand hygiene. • Provides complete access to fingers, hands, and wrists. • Wearing rings increases number of microorganisms on hands. • 2. Antiseptic hand rub: • A. Dispense ample amount of product into palm of one hand. • B. Rub hands together, covering all surfaces of hands and fingers with antiseptic. • Rub hands together until the alcohol is dry. Allow hands to completely dry before applying gloves.
Implementation – cont’d • 3. Hand-washing using regular or antimicrobial soap: • A. Stand in front of sink, keeping hands and uniform away from sink surface. (If hands touch sink during hand-washing, repeat sequence). • Inside of the sink is a contaminated area. Reaching over the sink increased risk of touching the edge, which is also contaminated. • B. Turn on water. Turn faucet on or push knee pedals laterally or press pedals with foot to regulate flow and temperature. • Knee pads within the operating room and treatment areas are preferred to prevent hand contact with faucet. Faucet handles are likely to be contaminated with organic debris and microorganisms. • C. Avoid splashing water against uniform. • Microorganisms travel and grow in moisture.
Implementation – cont’d • D. Regulate flow of water so temperature is warm. • Warm water removes less of protective oils on hand than hot water. • E. Wet hands and wrists thoroughly under running water. Keep hands and forearms lower than elbows during washing. • Hand are most contaminated parts to wash. Water flows from the least to the most contaminated area, rinsing microorganisms into the sink. • F. Apply 3 to 5 mL of antiseptic soap and rub hands together.
Implementation – cont’d • G. Perform hand hygiene using plenty of lather and friction for at least 15 to 20 seconds. Interlace fingers and rub palms and back of hands with circular motion at least 5 times each. Keep fingertips down to facilitate removal of microorganisms. • Soap cleans by emulsifying fat and oil and lowering surface tension. • Friction and rubbing mechanically loosen and remove dirt and transient bacteria. • Interlacing fingers and thumbs ensure that all surfaces are cleaned. • Adequate time is needed to expose skin surfaces to antimicrobial agent. • H. Areas underlying fingernails are often soiled. Clean them with fingernails of other hand and additional soap or with disposable nail cleaner. • CLINICAL DECISION POINT: Do not tear or cut skin under or around nail. • I. Rinse hands and wrists thoroughly, keeping hands down and elbows up.
IMPLEMENTATION – CONT’D • J. Dry hands thoroughly from fingers to wrists with paper towel, single-use cloth, or warm air dryer. • Drying from cleanest (fingertips) to least clean (wrist) avoids contamination. • Drying hands prevents chapping and roughened skin. • K. If used, discard paper towel in proper receptacle. • L. To turn off hand faucet, use clean, dry paper towel; avoid touching handles with hands. Turn off water with foot or knee pedals (if applicable). • M. If hands are dry or chapped, use a small amount of lotion or barrier cream dispensed from an individual use container. • Helps to minimize skin dryness. There is risk of organism growth in lotion, so only apply after patient care activities are complete.
evaluation • Inspect surface of hands for obvious signs of dirt or other contaminants. • Determines if hand hygiene is adequate.
Unexpected outcomes • 1. Hands or areas under fingernails remain soiled. • Repeat hand-washing with soap and water. • 2. Repeated use of soaps or antiseptics causes dermatitis or cracked skin. • Rinse and dry hands thoroughly after using soap and water; avoid excessive amounts of soap or antiseptic; try various products. • Use approved hand lotions or barrier creams. • Small individual use containers are preferred because large containers have found to harbor pathogens.
Special considerations • Instruct patient and family caregiver in proper techniques and situations for hand hygiene. • When patients are educated about the risks for infection, they play an important role in improving hand hygiene compliance in health care settings by reminding visitors and health care workers to perform hand hygiene.
Gerontologic considerations • The impact of infections is greater in older adults. • Hand hygiene by staff attending older adults is of utmost importance and should be an ongoing continuing-education requirement.
HOME CARE • Evaluate patient and primary caregiver to determine their understanding of the transmission of microorganisms and their ability and motivation to perform hand hygiene correctly. • Evaluate the hand hygiene facilities in the home to determine the possibility of contamination, proximity of the facilities to the patient, and the ability to maintain supplies and equipment.
End of skill • This is the end of the skill. • Your book has provided a video for this skill and the link is provided below: • http://booksite.Elsevier.com/Perry-Potter/ClinicalSkills/video07.php • Elsevier: Perry-Potter: Clinical Nursing Skills and Techniques, 8e – 7.1 Hand Hygiene Skill